Author:
Sophie Lindgren
Updated:
26 February, 2026
This chapter covers central venous catheters, including indications, insertion techniques, maintenance, and prevention of complications
- CVC – Insertion and Management
- Central Venous Catheter (CVC/C-line)
- CVC insertion in a patient treated with anticoagulant medication
- CVC insertion in patients with increased bleeding risk
- Use of ultrasound in CVC insertion
- Complications of CVC insertion
- Risk factors for complications during CVC insertion
- Choice of vessel for CVC insertion
- Venous Port (Port-A-Cath)
- Central Dialysis Catheter (CDC)
- Peripherally Inserted Central Catheter (PICC-line)
- CVC in Children
CVC – Insertion and Management
In Sweden, more than 30,000 central venous catheters (CVC/C-line) are inserted each year. CVC’s are placed to secure access to the bloodstream, which can be used over an extended period, usually 3-21 days. CVC’s are also used to measure central hemodynamics. Central venous catheterization has been described in scientific publications since the early 1900s, and catheter materials, insertion techniques, and uses have evolved over the past century. In modern healthcare, central venous catheters (CVC’s) are used for the safe administration of fluids, nutrition, and irritating medications. Their use is common in perioperative medicine and intensive care, as well as in dialysis medicine, surgery, pediatrics, and oncology. Although generally considered a safe method, CVC’s placement is associated with several mechanical and infectious complications.

A set with a four-lumen CVC, along with a scalpel, insertion needle, guidewire, and dilator in light blue. A white rubber vessel clamp for fixation at the skin level.
Central Venous Catheter (CVC/C-line)
CVC’s come in various lumen counts (1-5 lumens), with different lengths and thicknesses (F). A C-line is used for safe and reliable access to the bloodstream for 3-21 days. Typically, the subclavian vein or internal jugular vein is used. It is inserted with or without the aid of ultrasound. C-line is inserted via a skin puncture under local anesthesia in awake patients, without anesthesia in sedated or comatose patients. It can be tunneled or non-tunneled, with the latter being standard practice. A tunneled C-line is intended for long-term use, while a standard C-line should ideally not remain in place for more than three weeks.
A single-lumen standard C-line typically comes in lengths of 16, 20, or 30 cm with an outer diameter of 4, 5, or 6 French (F). The catheter is soft and radiopaque.
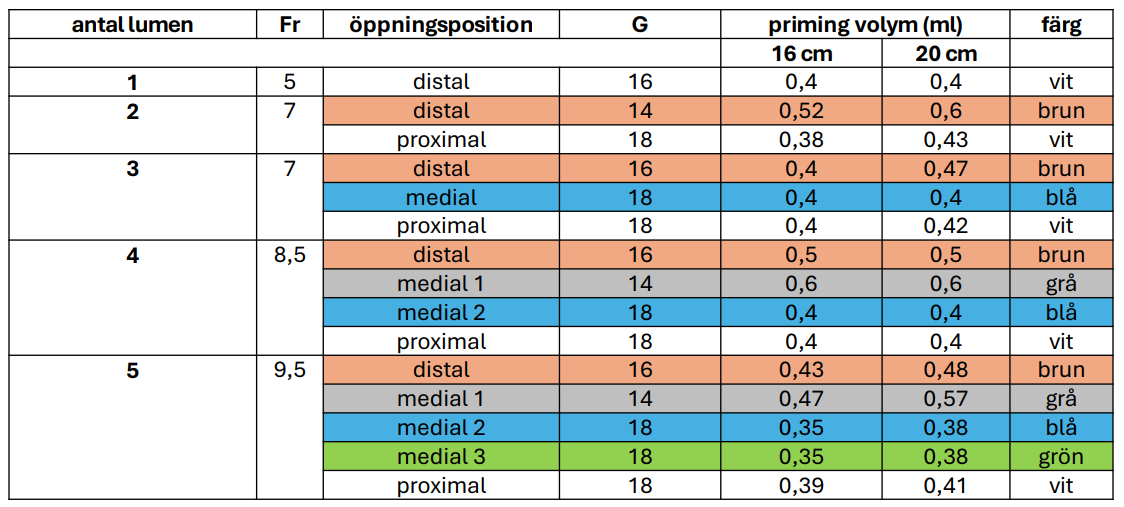
Dual-lumen and triple-lumen C-lines are typically available in 16, 20, or 30 cm lengths with an outer diameter of 7F. The catheter is soft and radiopaque. Four-lumen C-line have an outer diameter of 8F. Five-lumen C-line come in lengths of 16 or 20 cm with an outer diameter of 12F. In perioperative care and intensive care, multi-lumen C-line are generally used, typically opting for a 3, 4, or 5-lumen C-line.
The puncture needle may come with or without a plastic cannula. In some sets, you insert a metal needle and guide the wire through it, while in other sets, you first insert a plastic cannula (similar to a venflon), through which the guidewire is threaded. Another variant is the Y-shaped puncture needle, which allows the guidewire to be inserted through the side branch without removing the syringe used for blood aspiration (see image below).







CVC insertion in a patient treated with anticoagulant medication
If CVC insertion can wait and important treatment or monitoring is not delayed, anticoagulants should be discontinued before CVC placement. The procedure should then be postponed according to the guidelines below:
- Acetylsalicylic acid may be continued (no discontinuation)
- ADP receptor inhibitors
- ticagrelor (Brilique): postpone 3–5 days
- clopidogrel: 5 days
- prasugrel (Efient): 7 days
- DOAC
- apixaban (Eliquis): 12 hours
- edoxaban (Lixiana): 24 hours
- rivaroxaban (Xarelto): 24 hours
- dabigatran (Pradaxa)
- 12 hours with normal renal function
- 36 hours with impaired renal function
- Low molecular weight heparin
- if given as thrombosis prophylaxis: postpone 12 hours
- if given as treatment: postpone 24 hours
- Warfarin
- no action required (applies to INR values between 2 and 3)
CVC insertion in patients with increased bleeding risk
- A bleeding and coagulation history should be included in the evaluation prior to planned CVC insertion
- Laboratory testing with platelet count, INR, and aPTT is performed only if a coagulation disorder is suspected
- Prophylactic platelet transfusion is generally not required if platelets >20 × 10⁹/L
- Prophylactic plasma transfusion is generally not required if INR <3
- Patients with liver failure and elevated INR should not routinely receive FFP prior to CVC insertion
- Patients with sepsis-induced coagulopathy should not receive prophylactic procoagulants or platelet transfusions
- Routine discontinuation of anticoagulants or antiplatelet agents is not required
- For CVC insertion in patients with hemophilia, consultation with a coagulation specialist is recommended
- Insertion in patients with increased risk of bleeding complications should be performed in a
- compressible vascular site
- using ultrasound guidance
- by an experienced operator
- local anesthetic containing epinephrine should be considered
Use of ultrasound in CVC insertion
- Six RCTs, 2017–2022, 805 subclavian CVC insertions
- Real-time vs landmark technique
- Ultrasound increased success rate
- Ultrasound guidance increased first-attempt success
- Ultrasound guidance required fewer attempts for successful cannulation
- Ultrasound guidance was associated with shorter access time
- Ultrasound guidance was associated with lower complication rates
Pre-procedural overview ultrasound scan
- Assess the depth to the vessel and its relation to the artery, pleura, and nerves
- Assess vessel size, presence of thrombosis or stenosis, and respiratory variation
- Identify any aberrant vessels
- To select the most appropriate side
- Optimize ultrasound machine settings
Ultrasound-guided procedure
- Local anesthesia along the entire needle tract down to the vessel wall
- To avoid nerve injury
- To facilitate the procedure
- To reduce the risk of complications
- To detect and correct catheter malposition (e.g., into the internal jugular vein)
- To reduce the risk of CVC-related infection
Complications of CVC insertion
- Lund, Malmö, Helsingborg, Kristianstad, Ystad. March 2019 – December 2020, 12,667 CVC insertions
- Frequency of mechanical complications was 7.7% (95% CI 7.3–8.2)
- Frequency of serious complications 0.4% (95% CI 0.3–0.5)
- Bleeding grade 3–4
- Arrhythmia grade 3–4
- Arterial cannulation
- Permanent nerve injury
- Pneumothorax
- Ultrasound guidance was used in 93% of procedures
Risk factors for complications during CVC insertion
- BMI <20 kg/m2
- Male operator
- Limited operator experience (<100 CVC insertions)
- Number of skin punctures
- Increased risk of pneumothorax with subclavian vein access
Choice of vessel for CVC insertion
- Increased bleeding risk: femoral vein < internal jugular vein (possible airway compromise) < subclavian vein (non-compressible, possible life-threatening hemothorax)
- Risk of pneumothorax: internal jugular vein < subclavian vein
- Risk of catheter dysfunction: right internal jugular vein < femoral vein (thrombosis) < subclavian vein (thrombosis/stenosis/pinch-off) < left internal jugular vein (malfunction)
- Risk of infection: subclavian vein < internal jugular vein < femoral vein
- Patient comfort: subclavian vein > internal jugular vein > femoral vein
Choice of vessel for CVC insertion
- Perioperative short-term CVC – internal jugular vein
- ≥10 F catheter for adults (Certofix/CDK) – right internal jugular vein
- Outpatient CVC – subclavian vein
- Expected prolonged ICU stay – subclavian vein
- High risk of air embolism (e.g., hypovolemia + dyspnea) – femoral vein
- Risk of increased ICP – subclavian or femoral vein
- Unilateral lung pathology – ipsilateral subclavian/internal jugular vein
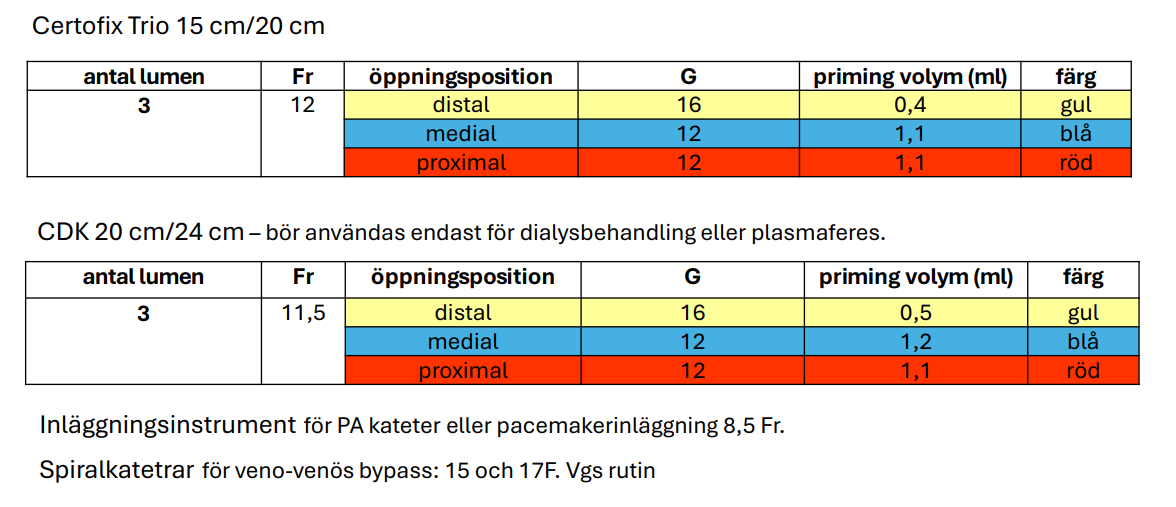
- Insertion instruments for PA catheter or pacemaker – right internal jugular vein or left subclavian vein
- Spiral catheters for veno-venous bypass – right internal jugular vein and femoral vein
Choice of CVC for high flow
- The larger the lumen diameter and the shorter the catheter, the higher the achievable flow.
- If high-flow transfusion is anticipated (viscosity!), a short and wide-bore central access should be chosen (e.g., Certofix)
- Certofix large lumens can be pressurized and are approved for contrast injection
- For administration of inotropes, choose
- a dedicated lumen
- with small internal dead volume (and low system compliance) to reduce the risk of fluctuations in circulatory parameters – usually high resistance is not problematic (pump-driven)
Choice of number of lumens in CVC
As a general rule, from an infection control perspective, a CVC with as few lumens as possible should be selected, but not at the cost of requiring additional peripheral lines, which in itself may increase infection risk.
Total parenteral nutrition requires a dedicated lumen that is not used for blood sampling or other medications.
Guidance for selecting number of lumens:
- 1 lumen – outpatient (chemotherapy) CVC, blood sampling/fluids/antibiotics on ward
- 2 lumens – TPN on ward
- 3 or 4 lumens – routine perioperative use
- 4 lumens – short expected ICU stay
- 5 lumens – prolonged ICU stay/complex clinical situation
- TPN in ICU – dedicated lumen of a multilumen CVC
- TPN on ward + blood sampling → 2 lumens
- Outpatient CVC – TPN + blood sampling → 2 lumens
- Outpatient TPN without blood sampling → one lumen (?)
Choice of CVC length
To determine the appropriate CVC length, measure the distance from the planned puncture site to the sternal angle. The sternal angle usually corresponds to the junction between the middle and lower third of the superior vena cava.
Commonly selected lengths:
- from right internal jugular vein: 16 cm
- from subclavian vein/left internal jugular vein: 20 cm
- in obese patients from subclavian vein: possibly 30 cm
Connections of CVC lumens (ports) perioperatively
- Distal lumen brown – CVP monitoring
- Medial lumen blue – vasopressors and inotropes
- Medial lumen gray/green – other fluids and medications
- Proximal lumen white – anesthetic agents
Suturing of CVC
- The CVC is secured with monofilament suture.
- If the CVC has not been inserted to its full length, it should always be secured with sutures in both the flexible and the fixed wings.
- If the CVC has been inserted to its full length, secure it with two sutures in the fixed wing and one suture in the groove closer to the insertion site.
Locks in the lumens
In general, it is recommended to flush the catheter lumens with 20 ml NaCl 0.9% using a pulsatile technique after CVC insertion. For dialysis catheters, after flushing with NaCl, a citrate lock with sodium citrate 46.7% (Citratflow or DuraLock-C) is recommended in a volume corresponding to the priming volume of the large lumens.
Injection membranes
Each lumen should be fitted with a positive displacement connector (e.g., Caresite Braun) or a neutral connector (e.g., Bionector Vygon). Negative displacement connectors or check valves should not be used on CVCs.
Dressing
The catheter is covered with a highly permeable polyurethane dressing intended for CVCs, with the insertion site clearly visible through the transparent window. The dressing must be sealed without air channels to the insertion site. For improved fixation and skin protection, Cavilon may be applied.
Optimal position
- Theoretically, the optimal catheter tip position with the lowest risk of complications or dysfunction is in the lower part of the superior vena cava or in the right atrium
- Routine chest X-ray after CVC insertion into the internal jugular vein
- for expected short-term use
- without suspicion of mechanical complications is not recommended.
CVC must be X-rayed if:
- CVP monitoring
- chemotherapy treatment
- CDK insertion
- complicated insertion
Exchange over guidewire
- Catheter exchange over a guidewire may be performed if the insertion site shows no signs of irritation and there is no suspicion of CVC-related infection.
- Guidewire exchange may be considered in case of catheter dysfunction or change of catheter type and likely carries a lower risk of mechanical complications without a higher risk of infection.
- Guidewire exchange should, if possible, be performed under the same sterile conditions as a new insertion but should be avoided in the presence of an infected insertion site or strong suspicion of CVC-related infection.
- The optimal technique for guidewire exchange is insufficiently studied.
- Since the external portions of a CVC are more frequently colonized with microorganisms than the subcutaneous and intravascular parts, one should avoid advancing the guidewire from the external part of the catheter.
- Various techniques aimed at avoiding this step are considered risky.
- Therefore, guidewire exchange should only be considered when the risk of mechanical complications from a new insertion is higher than the risk of catheter-related infection
- Should if possible be avoided in:
- long-standing indwelling central venous catheter
- exchange from a larger-lumen catheter to a smaller-lumen catheter (remaining open, “tunneled” connection to the vein)
Venous Port (Port-A-Cath)
Designed for long-term use (> 3 weeks), the Port-A-Cath is inserted percutaneously or via a small incision in the subclavian or jugular vein under local anesthesia or general anesthesia. It is used primarily for long-term administration of chemotherapy. The port’s membrane is accessed through the skin using a short needle (Gripper needle) into the port chamber.
The insertion of a Port-A-Cath is typically performed under general anesthesia. The procedure may be done by a surgeon or an anesthesiologist, often in collaboration. It begins with gaining vascular access in the internal jugular vein on the neck, using ultrasound for guidance. A long guidewire (e.g., 150 cm Terumo wire) is then placed into the vena cava, and its position is confirmed using fluoroscopy. An incision is made near the sternum (usually on the left side), and a tunneling instrument is passed subcutaneously from the insertion site to the port’s location. The Port-A-Cath catheter is threaded over the guidewire and placed about 2-3 cm below the carina and approximately 15 cm from the insertion site. The area for the port is prepared by dilating the space next to the sternum, where the port is secured with deep sutures to the underlying muscle, using 4-0 Prolene. Two additional sutures are used for fixation. Blood flow in the tunneled catheter is tested, and the port is then connected. Subcutaneous and skin sutures are placed with individual Dermalon stitches. The port’s function is checked with a Gripper needle to ensure that blood can be aspirated and saline can be injected. The entire system is filled with 4 ml of heparin solution (100 units/ml). The neck incision is sutured with 3-0 Dermalon, and local anesthesia is administered at the port site. A final x-ray check is performed to confirm placement, and simple dressings are applied to the neck and port sites.

Central Dialysis Catheter (CDC)
CDC are used for large transfusions or dialysis treatment. They can be inserted as tunneled or non-tunneled catheters for dialysis. Most often, CDC insertion is ultrasound-guided and percutaneous (via a skin puncture with a small incision) under local anesthesia in the subclavian vein, jugular vein, or groin. Tunneled CDC are designed for long-term use, while non-tunneled CDC are used acutely and should not remain in place for more than three weeks. CDC are thicker than regular CVC, typically available in lengths from 20 to 35 cm and diameters ranging from 13.5F to 15.5F. CDC typically have two lumens, although some have three lumens, such as those used for citrate dialysis. A CDC for citrate dialysis may be thinner than one for hemodialysis, as it requires lower blood flow, usually 13.5F. If a CDC is placed in the groin, a longer catheter, typically 28-35 cm, should be used. Due to the thickness of the CDC, a small incision with a scalpel facilitates dilation before catheter insertion. Dilation is usually performed with two dilators of different sizes before the catheter is inserted into the vessel. A CDC must always be x-rayed before use.
The right internal jugular vein is the first choice for ICU patients and acute patients due to the lower risk of mechanical complications (e.g., pneumothorax) and generally good accessibility. The right side offers a more direct route centrally than the left and avoids the risk of damaging the thoracic duct. Note that the infection risk is higher with a catheter in the groin, especially in men, and patients with an expected need for a catheter are best suited for the right internal jugular vein (e.g., temporary dialysis catheter or VV-ECMO cannula). If possible, avoid placing a CVK in the same vessel.
Peripherally Inserted Central Catheter (PICC-line)
PICC stands for Peripherally Inserted Central Catheter. It is placed under ultrasound guidance and percutaneously through a vein in the upper arm, typically the basilic vein. These catheters are intended for both short- and long-term use. The catheter is inserted into a peripheral vein in the upper arm, with the tip positioned in the superior vena cava/right atrium or at the cavoatrial junction. PICC lines are mainly used for long-term intravenous treatment, typically lasting 1 to 6 months, making it an alternative to other central venous catheter systems such as Portacath.


), chronic dialysis treatment, intensive care, and when chemotherapy is administered repeatedly over long periods.
Insertion of Central Venous Catheter
Careful preparation during central venous catheter placement can reduce the risk of complications. It is important to have a good understanding of local anatomy and anatomical variations, select the appropriate vessel, choose the suitable catheter type, maintain sterility, use a minimally invasive technique, and call for help when problems arise or if inexperienced, have help readily available.
CVC catheters come in different lengths, typically 16 or 20 cm, and with varying lumen counts, between one and five lumens. A single-lumen catheter is most commonly used for intravenous access in regular hospital wards, while 3-5 lumen catheters are used for multiple accesses in ICU. Longer catheters, 30-35 cm, are needed for placement in the groin.

Maximally Sterile Concept
When inserting central venous catheters, the “maximally sterile concept” should be applied. This involves creating the same conditions as during surgery to minimize the risk of catheter contamination before or during its insertion into the bloodstream. See the image series below.

Vessel Selection
When selecting a vessel, consider what the catheter will be used for, how long it will remain in place, the risk of complications, and the patient’s anatomy at the insertion sites. Is the patient prone to bleeding? Does the patient have lung disease, a history of radiation therapy, or implanted vascular grafts? Will the patient receive chemotherapy or other irritating or cardiotoxic substances? Is the catheter intended for dialysis? Is the patient immunosuppressed? What is most comfortable for the patient?
Internal Jugular Vein
This is the first choice in many clinics for CVC insertion. The vessel is easy to visualize with ultrasound, and the risk of lung injury is considered lower. In case of vessel damage or bleeding, the veins in the neck can be compressed. It can also be used for long-term access, but preferably through tunneling due to a higher risk of infection compared to the subclavian vein.
External Jugular Vein
This vessel’s anatomical course is more superficial and somewhat more tortuous than the internal jugular vein, but it is easy to visualize with ultrasound and is a valid alternative, especially when other vessel locations are unsuitable for various reasons. Long-term access via this vessel is uncommon.
Subclavian Vein
This vessel is often used for both long-term and short-term access. It is somewhat more challenging to visualize with ultrasound than the internal or external jugular veins because it runs under the clavicle, but using a lateral puncture technique (puncture as close to the shoulder joint as possible), good visibility is possible. The vessel is easy to identify using the landmark technique in most cases. The risk of pneumothorax is obviously higher than for other vessel locations. In the event of a vessel injury with significant bleeding, it is not possible to compress this vessel due to its anatomical course. However, studies have shown that puncturing the subclavian vein does not cause more severe vascular injuries compared to puncturing the veins in the neck. If you are an inexperienced CVC inserter or have had difficulties during insertion (more than three attempts), it is advisable to perform a chest X-ray afterward.
Axillary/Basilic Veins
These vessels run in the forearm and can easily be visualized with ultrasound. They have a significantly smaller diameter than central veins and the femoral vein and are used for the insertion of PICCs (Peripherally Inserted Central Catheters) and other types of longer catheters known as “half-way” or “mid-line” catheters. A PICC reaches all the way to the superior vena cava. The advantage of using these vessel locations is that there is no risk of complications such as pneumothorax or severe vascular injuries during insertion. However, studies have shown that the risk of thrombosis is higher. A position check of the catheter tip with, for example, a chest X-ray is appropriate.
Femoral Vein
This is a large vessel that is easy to visualize with ultrasound just below the inguinal ligament. It usually lies just medial to the femoral artery, but anatomical variations are common. This vessel location is not suitable for long-term access because the catheter will be close to the hip joint. The risk of infection is also higher for catheters placed here. This vessel is most often used in cases of severe illness/trauma and major surgical interventions, especially when the patient is prone to bleeding or when other vessel locations are unavailable for various reasons.
Insertion Technique and Catheter Material
There are various materials and techniques for inserting a catheter into the central bloodstream. Some techniques and materials are used in emergency situations when it may be difficult to maintain full sterility. In such cases, it is important to extract or replace the catheter as soon as the patient is stabilized. In planned catheter insertions, a maximally sterile concept should always be applied, regardless of which vessel, type of catheter material, or puncture technique is used.

Catheter over Needle (Seqalon T)
In emergency situations when quick access to the bloodstream is required, slightly stiffer Teflon catheters can be used, which sit directly over a slightly longer puncture needle. This eliminates the need for a guidewire to insert the catheter into the bloodstream. These catheters have a larger inner diameter and are shorter than catheters inserted over a guidewire. This allows for rapid fluid infusion and transfusion of blood products. These catheters are not intended for permanent use and should be removed as soon as possible. The long needle increases the risk of vascular and thoracic injuries during central puncture.
Catheter over Guidewire (Seldinger Technique)
Sven-Ivar Seldinger was a radiologist from Mora in Sweden who invented the technique of percutaneous catheter insertion into the bloodstream over a guidewire that had been inserted into the blood vessel via a needle. The technique requires dilating the surrounding tissue and vessel wall before inserting the catheter (see image series below). The technique made it possible to use longer and softer catheters made of silicone or polyurethane without first exposing the vessel. This reduced the risk of both infectious and mechanical complications.
Catheter over Guidewire via Insertion Instrument (Modified Seldinger Technique)

A variation of the Seldinger technique is used for the insertion of venous ports, tunneled CVKs, PICCs, pulmonary artery catheters (PA), and interventional radiology catheters. The difference is that an insertion instrument is placed over the guidewire, the guidewire is removed, and the catheter is then inserted through the lumen of the insertion instrument.
Landmark-Guided Puncture

Traditionally (before the ultrasound era), vessel identification for puncture was done solely using anatomical landmarks and palpation of nearby arteries. Once the vessel was identified, fluoroscopy with contrast could be used to confirm the location. However, the most common approach was to perform the entire catheterization using only landmarks and palpation. When straightforward, landmark-based insertion is quick, but with anatomical variations and degenerative vessel changes, there is a higher risk of complications with multiple punctures, increasing the risk of pneumothorax and vascular injury. Even with ultrasound-guided puncture, knowledge of anatomical landmarks is still very helpful. When quick access to a central line is needed, such as in prehospital care, the landmark technique remains useful.
Ultrasound-Guided Puncture

Over the past ten years, advancements in ultrasound equipment have made the technique significantly easier to use, and ultrasound-guided puncture is now the first choice for central line insertion. Studies have shown that ultrasound-guided puncture reduces the number of CVC-related insertion complications. With the ultrasound probe oriented longitudinally along the vessel to be punctured, the depth to the vessel and the needle’s entry into the vessel can be monitored throughout the procedure (“Longitudinal Axis-In Plane” procedure, LAX-IP). The use of ultrasound-visible needles is recommended, as it is more difficult to assess the needle tip’s position using surrounding tissue movements. This reduces the risk of injury to vessels, nerves, the pleura, and other surrounding tissue. For an experienced user, ultrasound-guided puncture does not take longer, but the technique requires a learning period.
Position Verification
Verification of the catheter tip’s position is recommended when inserting long-term systems and when the catheter is to be used for the administration of cytotoxic, vasoactive, and irritating medications. The most common way to verify the tip position is with a chest X-ray or fluoroscopy via a C-arm immediately after insertion. The catheter tip should be located in the distal superior vena cava or at the atrial junction.


Documentation Upon Insertion
Accurate documentation of central venous catheter (CVC) insertion is essential for tracking potential complications. Follow-up on central line placements is crucial to maintain patient safety and implement quality improvements in healthcare. We are legally obligated to document and continuously improve the quality of procedures that pose risks to patients (SOSFS 2008:1, 2011:9, 2013:6). There are international recommendations for what should be documented during central line insertion. A minimum requirement includes the indication, catheter type, number of lumens, vessel choice, insertion technique (ultrasound or not), number of punctures (complicated or uncomplicated), depth of the catheter in the skin, and whether an X-ray check is necessary. Using a checklist during insertion helps maintain patient safety. The idea originates from the aviation industry and has resulted in a CVC checklist developed by “Dr. Checklist” Peter Pronovost at Johns Hopkins Hospital in Maryland, USA. This checklist was adapted at Sahlgrenska University Hospital in 2010 for Swedish conditions and has been recently updated. See image below.

Extraction of Central Venous Catheter
When the catheter is no longer needed, or if there is a suspected CVC-related infection, the catheter should be removed promptly. Documentation of the extraction should be made in the patient’s medical record. If an infection is suspected, the catheter tip should be sent to bacteriology for culture testing. If the infection is suspected to have spread to the bloodstream (catheter sepsis), peripheral blood cultures should also be taken and sent to bacteriology. It is important to request the blood culture incubation time on the referral to compare the time to bacterial growth between peripheral blood samples and those drawn from the CVC. Faster bacterial growth in the CVC sample suggests the infection originated from the catheter. Antibiotic treatment should be initiated or adjusted in consultation with an infectious disease specialist. A catheter that has been in place for a long time may become stuck in the vessel due to thrombosis and fibrin formation. If the catheter material is known or suspected to be adhered to the vessel, vascular surgery and interventional radiology specialists should be consulted before extraction.
Complications
A wide range of complications can occur with central venous catheters. These are generally categorized as “Mechanical and Infectious Complications.” Mechanical complications include vascular/thoracic injuries, catheter misplacement, catheter dysfunction, and loss of guidewires or catheter materials into the bloodstream. Infectious complications include local skin and soft tissue infections at the insertion site, as well as catheter-associated bloodstream infections. Although these complications are rare relative to the vast number of catheter days, they cause significant patient suffering, death, and increase healthcare costs. Inserting catheters via central veins in the neck and thorax can cause life-threatening bleeding, pneumothorax, and pericardial injury. PICCs are not associated with these serious insertion complications as they are inserted through smaller veins in the upper arm. The longer a catheter remains in place, the higher the risk of microbial colonization and bloodstream infections. There is some uncertainty regarding the infection and thrombosis risks associated with different types of central venous catheters. The larger and longer the catheter, the greater the risk of thrombosis in the vessel where the catheter is placed. Data suggests that PICCs and large dialysis catheters may cause more thrombosis than other catheter types. In terms of infection risk, evidence suggests that venous ports and tunneled CVC are the best options, as they are placed under the skin, minimizing the risk of bacterial contamination during use, care, and maintenance.
Mechanical Complications
Serious complications are rare compared to the large number of catheter days, ranging from 5-80 events per 10,000 catheter days in published studies. However, the consequences for affected patients are significant. Examples of mechanical complications include catheter tip mispositioning, catheter dysfunction, guidewire/catheter materials being lost in the bloodstream, thrombophlebitis with pulmonary embolism, pneumothorax, vascular injuries, and arrhythmias. It is crucial to be aware that serious complications can occur during CVC insertion and to manage them swiftly by contacting vascular, radiology, or thoracic surgery specialists. Mechanical complications can be minimized by optimizing conditions during CVC insertion. Access to ultrasound and fluoroscopy is recommended, as are surgical-like sterile conditions. Using a checklist during CVC insertion also helps to prevent complications (see image above).
Infectious Complications
Invasive bloodstream infections vary among patient groups, ranging from 0 to 30 per 1,000 catheter days. Infectious complications cause extended hospital stays, increased healthcare costs, patient harm, and death. Central venous catheter-related infections (CRI) are a major cause of iatrogenic morbidity and mortality. Across all patient categories, the incidence of CRIs varies from near zero to 30 per 1,000 catheter days, depending on the care unit. Intensive care units (ICU) tend to have higher CRI rates. Mortality varies from zero to 35 percent in various studies. Hospital stays may be extended by 10-20 days, and 12 percent of all infections acquired in intensive care are related to central venous access. Several studies show that simple measures can significantly reduce the incidence of these infections. If an infection is suspected, the catheter tip should be sent for culture testing. If the infection is suspected to have spread to the bloodstream (catheter sepsis), peripheral blood cultures should also be taken. It is crucial to request the incubation time on the culture request to compare the time to bacterial growth between peripheral and CVC blood samples. If bacterial growth is faster in the CVC sample, the infection likely originates from the catheter. Antibiotic treatment should be started or adjusted in consultation with an infectious disease specialist.
Follow-up, Education, and the Importance of Vascular Access Centers
There is strong evidence that follow-up on CVC complications is important to prevent them from occurring. There are many evidence-based measures that healthcare personnel must follow to reduce the risk of complications during CVC insertion and use. Continuous monitoring of CVC complications and feedback to the clinical team are essential to motivate healthcare personnel to follow these evidence-based procedures. Organized training in CVC insertion and management is also critical to minimize all types of complications. Ultrasound-guided puncture reduces the risk of mechanical complications during insertion. Radiographic verification after complex insertions or to check catheter tip placement allows for early detection of mechanical complications.
Establishing local vascular access centers is considered to greatly improve care quality and patient safety during CVC insertion and management. Concentrating vascular access expertise in a few individuals optimizes the physical and technical conditions for catheter insertion. It also facilitates local follow-up of centrally inserted venous catheters at a clinic or hospital.
References CVC
- Frykholm et al. Clinical guidelines on central venous catheterization (2014) ACTA Anaesth Scand
- Lindgren et al. Survey of central venous catheterization practice in Sweden (2013) ACTA Anaesth Scand
- Pikwer et al. Complications associated with peripheral or central routes for central venous cannulation (2011) Anaesthesia
- Silberzweig et al. Reporting standards for central venous access (2003) J Vasc Interv Radiol
CVC in Children


Central Venous Access
- Do not hesitate to place a CVC in sedated children! Awake children are trickier…
- Check for any echocardiogram results, especially in children with syndromes (systemic vein anatomy)
- The technique is similar to adults for older children (> 10 kg)
- Choose a vessel you’re comfortable with – for smaller children, v. jug. int. dx. is the safest option
- Aim the catheter tip at the right atrium or the superior vena cava/right atrium junction
- Use fluoroscopy if unsure
Central Venous Access – Smaller Children
- When you get backflow, remove the syringe and release the needle
- Check that blood is still flowing back from the needle
- Use Nitinol guidewires (already included in smaller CVC sets made by Arrow) – it’s safer and increases success rates
- Unwind the guidewire from the plastic loop before starting
- For smaller children, use the straight end first (the bend won’t fit into the vessel)
- Be gentle when advancing the guidewire
CVC Size (Central Venous Catheter/C-line)
- < 10 kg: 3-5 fr/4-6 cm
- 10-30 kg: 5-6 fr/6-8 cm
- > 30 kg: 7 fr/10-16 cm
| Weight | CVL Sizes | Catheter length |
|---|---|---|
| <10 kg | 3–5 French | 4–6 cm |
| 10–30 kg | 5–6 French | 6–8 cm |
| >30 kg | 7 French | 10–15 cm |
CVC Depth – IJV dx (cm)
- 1.7 + (0.07 x height in cm)
