Author:
Kai Knudsen
Reviewer:
Sven Erik RickstenUpdated:
20 February, 2026
Here, circulatory failure and heart failure are described, along with monitoring and treatment using inotropic and blood pressure-raising agents. Commonly used drugs, their effects, and appropriate dosing are briefly described here.
- Circulatory Failure and Blood Pressure Raising Treatment
- Heart Failure – Perioperative Management
- Cardiomyopathy
- Inotropic Drugs
- Pulmonary Hypertension
- Treatment of Heart Failure with Inotropic and Vasoactive Drugs
- Inotropic and Vasoactive Drugs in Cardiogenic Shock
- Guidance in the treatment of chronic heart failure with reduced systolic left ventricular function
- Individualized Treatment According to Clinical Presentation
- Management of Persistent Symptomatic Heart Failure
- Additional Important Measures
- Antiarrhythmic Drugs – Vaughan Williams Classification
- Class I – Sodium Channel Blockers (Na⁺)
- Class II – Beta Blockers
- Class III – Potassium Channel Blockers (K⁺)
- Class IV – Calcium Channel Blockers (Ca²⁺)
- Adrenaline (Epinephrine)
- Argipressin
- Dobutamine (Dobutamine Hameln®)
- Dopamine (Giludop®)
- Ephedrine
- Levosimendan (Simdax®)
- Phenylephrine
- Milrinone (Corotrop®)
- Isoprenaline
- Nitroglycerin
- Norepinephrine
- Vasopressin
- Cordarone (Amiodarone)
- Corotrop (Milrinone)
- Simdax (Levosimendan)
- Remodulin (Treprostinil)
- Ventavis (Iloprost)
Circulatory Failure and Blood Pressure Raising Treatment
Inotropic treatment refers to intravenous vasopressor treatment with potent short-acting vasoactive drugs. The commonly used drugs are synthetic fast-acting catecholamines. These medications are administered intravenously, either intermittently or continuously, via a central venous catheter (CVC) or a peripheral venous cannula (PVC). The treatment usually, but not always, results in elevated blood pressure, increased cardiac output, and improved oxygen transport. Catecholamines activate α and β receptors in vital organs and peripheral vessels. Αlpha1 receptors are mainly found in peripheral blood vessels postsynaptically, β1 receptors are predominantly in the heart, β2 receptors are present in the heart, blood vessels, uterus, and airways. DA1 receptors are primarily found in the splanchnic region and kidneys. Vasopressors have short-term sympathomimetic effects on circulation, improving blood pressure and oxygen delivery, but prolonged use may risk damage to vessels, extremities, and vital organs like the heart and kidneys. There is an increased risk of arrhythmias and ischemia, though the risk depends on how the drugs are used. Common vasopressors include dopamine, adrenaline, noradrenaline, and dobutamine. Long-term use may lead to a tired heart with heart failure and increased risk of intestinal ischemia and peripheral ischemia. For moderate blood pressure drops, short-acting drugs like ephedrine and phenylephrine are recommended initially. If longer effects are needed, continuous infusion of more potent drugs is recommended.

Suggestions for treating hypotension that does not respond to initial fluid administration: For a low pulse < 90 bpm and low blood pressure: First-line therapy is ephedrine 5-10 mg IV, second-line therapy is dopamine 2-10 μg/kg/min, dosed based on pulse and blood pressure response. Third-line therapy is adrenaline 0.1-1.0 mg IV, followed by continuous infusion 0.05-0.1-0.30 μg/kg/min, dosed according to pulse and blood pressure response. For a high pulse > 90 bpm and low blood pressure: First-line therapy alongside fluid therapy is phenylephrine 0.1-0.2 mg IV, second-line therapy is dobutamine 2-10-15 μg/kg/min or noradrenaline, dosed based on pulse, blood pressure, CO, and SvO2. Noradrenaline is given via continuous infusion at 0.01-0.1-(0.5) μg/kg/min = 3-40 ml/h for a 70 kg patient. The usual starting dose of noradrenaline is 0.05 μg/kg/min, dosed based on blood pressure. Noradrenaline can also be used as a first-line drug for critically ill patients but should ideally not be administered via a peripheral venous cannula due to the risk of hemodynamic instability.
Physiological Effects of Inotropic Drugs
| Inotropic Agent | α 1 | β 1 | β 2 | DA- 1 | SVR | CO | HR | BP |
|---|---|---|---|---|---|---|---|---|
| Epinephrine | ++++ | ++++ | +++ | ↑ | ↑ | ↑ | ↑ | |
| Norepinephrine (Noradrenaline) | +++ | +++ | + | zero | ↑ | +/- | ↑ | ↑↑ |
| Dobutamine | + | ++++ | ++ | zero | ↓ | ↑ | ↑ | +/- |
| Dopamine | ++ | ++++ | ++ | +++ | ||||
| Ephedrine | + | +++ | ++ | zero | ||||
| Phenylephrine | +++ | zero | zero | zero | ||||
| Isoprenaline | zero | ++++ | ++++ | zero | ||||
| Levosimendan | ↓ | ↑ | ↑ | ↓ | ||||
| Milrinone | ↓ | ↑ | ↑ | +/- | ||||
| Vasopressin | +++ | +++ | + | zero | ↑ | +/- | ↑ | ↑↑ |

Low Blood Pressure and Inotropic Drugs
| Low blood pressure (< 90 mmHg) and low heart rate (<80 beats/min) | Low blood pressure (< 90 mmHg) and high heart rate (>80 beats/min) | |
|---|---|---|
| First choice medication for immediate effect | Ephedrine 5-10 mg i v. intermittently | Phenylefrine 0,1 mg i v. intermittently |
| Choice of moderate continuous medication | Dopamine 2-10-15 μg/kg/min | Phenylefrine in continuous infusion, 0,05-0,15 μg/kg/min |
| Choice of strong continuous medication | Epinephrine 0,01-0,1-(0,5) μg/kg/min | Norepinephrine in continuous infusion, 0.01-0.1- (0.5) μg /kg/min |
Heart Failure – Perioperative Management
Chronic Heart Failure
- Prevalence ≈ 2%
- > 75 years, prevalence ≈ 8 %
- Within 10-20 years, the prevalence has increased 2-3 times
- Increased age
- Today, more people survive acute infarction but develop heart failure
Chronic Heart Failure – Clinical Syndrome
- Reduced ventricular function
- Increased pressure in the pulmonary circulation
- Reduced physical capacity
- Neuroendocrine activation
- Reduced survival

Pathophysiology of Heart Failure
- (MAP – CVP) = Cardiac output x SVR
- Cardiac output = SV x HRSV ↓ CO ↓






Pharmacological Treatment
- ACE inhibitors
- Angiotensin II receptor blockers
- β-blockers (metoprolol, bisoprolol, carvedilol)
- Aldosterone receptor antagonists
- Digoxin
ACE inhibitors, angiotensin II rec. blockers
- Reduces angiotensin II
- Reduced catecholamines
- Reduced aldosterone
- Reduced ADH
- Increases bradykinin
- Increases NO
- Increases MPGI2
- Reduced production of tissue angiotensin II
- Antiproliferative effect
- Reduces remodeling
β-blockers (metoprolol, bisoprolol, carvedilol)
- Reduces MVO2
- Increased glucose uptake
- Improved energy utilization
- Antiarrhythmic effect
- Reduced Ca2+ leakage from SR
- Antiapoptotic effect
- Antioxidant
Aldosterone receptor antagonists
- Reduced myocardial collagen
- Lowers catecholamines
- Improves baroreflex
- Improves endothelial function (NO)






Brain Natriuretic Peptide (B-type natriuretic peptide, BNP)
- Produced in the left ventricle and released upon ventricular wall distension (increased preload)
- Released together with NT-proBNP, which is biologically inactive
- Vaso-venodilation, increases GFR, natriuresis, inhibits RAAS
- Longer half-life than ANP
Prognostic Value of Natriuretic Peptides (BNP, NT-proBNP)
- Preoperative elevation of BNP/NT-proBNP increases the risk for:
- MACE (OR: 19.8)
- Mortality (OR: 9.3)
- Cardiac death (OR: 23.9)
- “Cut-off” level?
- Method
- BNP/NT-proBNP in relation to other methods?

NT-proBNP Reference Values
- < 400 ng/l heart failure unlikely
- 400-900 ng/l possible heart failure
- > 900 heart failure likely
Perioperative Management
- Identification of high-risk patient (EF, NT-proBNP, clinic)
- Is the patient optimally treated for heart failure?
- What do we do with “heart failure medication” before surgery?
Pharmacological Treatment
- ACE inhibitors, angiotensin II receptor blockers
- β-blockers (metoprolol, bisoprolol, carvedilol)
- Aldosterone receptor antagonists
- Diuretics
- Digoxin
Perioperative Management
- Identification of high-risk patient (EF, BNP, clinic)
- Is the patient optimally treated for heart failure?
- What do we do with “heart failure medication” before surgery?
- Choice of anesthesia technique (regional, general anesthesia?)
Surgery in Lower Body
Regional anesthesia in primary heart failure and heart failure secondary to:
- Aortic insufficiency
- Mitral insufficiency
Cardiomyopathy

Case Report
- 37-year-old woman with twin pregnancy at week 33. Seeks emergency care due to shortness of breath and leg swelling. Previously heart-healthy.
- BP: 110/60, HR: 120, SpO2 90%
- Slight elevation of CK-MB. ECG: repolarization disturbance.
- Echo shows biventricular failure. LVEF: 20% MI, TI grade 3/4.
- Treatment started with furosemide and nitroglycerin infusion
Decision for emergency C-section. Anesthesia technique?
Anesthesia Induction in Heart Failure
- Hypnotics:
- thiopental
- midazolam
- ketamine
- propofol
- Opioids (fentanyl)
Hemodynamic effects of Anesthetics
| Anesthetic Agent | Negative inotropic effect | Vasodilatation | Filling pressure | Heart rate |
|---|---|---|---|---|
| Propofol | yes | yes | reduces | varies |
| Fentanyl | no | yes | reduces | reduces |
| Ketamin | ? | no | increases | increases |
| Isoflurane | yes | yes | unchanged/increases | increases |
| Sevoflurane | yes | yes | unchanged/increases | increases |
| Midazolam | yes | yes | reduces | increases |
Anesthesia Induction with Propofol (2 mg/kg + 0.1mg/kg/min) and its Effects on Muscle Sympathetic Activity (MSA), MAP, and HR

Maintenance of Anesthesia
- TIVA (propofol, opioid)
- Inhalation anesthesia
Intraoperative Monitoring in Heart Failure
- Invasive blood pressure
- 2-3 lead ECG, ST trend
- CVC
- PA catheter?
- TEE – in case of severe hemodynamic instability
Inotropic Drugs
- Adrenaline
- Noradrenaline
- Isoprenaline
- Dopamine
- Dobutamine
- Phosphodiesterase inhibitors
- amrinone
- milrinone
- enoximone
- Calcium sensitizers
- levosimendan

Inotropic Drugs
- Noradrenaline (Norepinephrine)
- Adrenaline (Epinephrine)
- Dopamine
- Dobutamine
- Isoprenaline
- Levosimendan
- Milrinone

Recommendations
- Identify high-risk patient
- Arterial line, CVC (the day before)
- Monitor arterial pressure (MAP), central venous saturation before induction
- Connect milrinone and noradrenaline (NA) to CVC
- Use anesthesia technique you are familiar with
- Maintain MAP (65-75 mmHg) with NA
- Maintain central venous saturation (≈ 60-70%) with milrinone
- Administer fluids based on CVP
- Hemoglobin > 100 g/l
- Have two anesthesiologists at the start of anesthesia!
Diastolic Heart Failure
- Myocardial relaxation
- Active, energy-requiring process
- Affected by ischemia and
- Inotropic drugs
- Passive filling
- Extracardiac factors
- Structural factors

Diastolic Dysfunction
Definition:
- Normal filling pressure results in inadequate filling of the LV
- Elevated filling pressure is required for adequate LV filling
- 40-50% of heart failure patients have isolated diastolic dysfunction
Isolated Diastolic Dysfunction
- Hemodynamics similar to systolic failure
- LVEF is normal, LVEDV low
- LV hypertrophy
- Abnormal mitral Doppler (E/A <1)
- Hypertension, aortic stenosis
- Dynamic LV outflow obstruction (functional aortic stenosis)


Treatment of LV Outflow Obstruction with SAM
- Increase preload (“volume challenge”)
- Avoid tachycardia
- No inotropic agents
- No vasodilators
- In case of tachycardia, administer β-blockers
- Guide therapy with echo-Doppler!!!



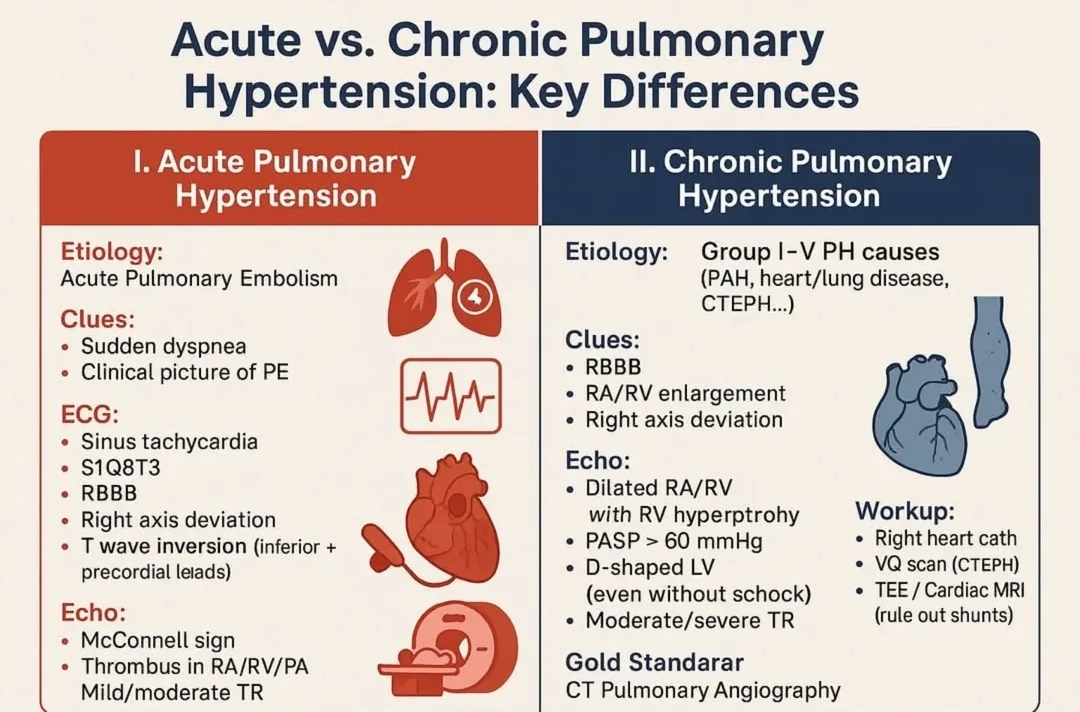
Pulmonary Hypertension
- MPAP > 25 mmHg or SPAP > 55 mmHg
- Right ventricular hypertrophy/failure
- Classification:
- Pulmonary arterial hypertension
- Primary, idiopathic pulmonary hypertension (sporadic, familial)
- Related to collagen vascular diseases (scleroderma, lupus, RA)
- Portopulmonary hypertension
- Pulmonary venous hypertension (LV failure, MI/MS, AS)
- Pulmonary hypertension associated with lung disease
- Pulmonary hypertension caused by thromboembolism
- Pulmonary arterial hypertension
Pulmonary Hypertension and Right Ventricular Failure
The Pulmonary Circulation and Right Ventricle


Interaction between RV and LV (“ventricular interdependence”)
- Changes in pressure/volume in one ventricle directly affect the pressure/volume in the other ventricle
- Immediate force transmission between RV and LV
- Shared muscle fibers, septum, pericardium
- Diastolic and systolic interaction

Diastolic Ventricular Interaction with RV Pressure/Volume Loading
- Increased volume/distension of RV during diastole, septum shifts to the left
- Reduces LV volume, i.e., reduced LV preload
- LV end-diastolic pressure (PCWP) increases
- LV compliance decreases


Systolic Ventricular Interaction with RV Pressure/Volume Loading
- With RV pressure/volume loading, a flattened septum shifts from left to right during systole
- LV assist is more effective at high systemic pressure
- RV function deteriorates at low systemic pressure (peripheral vasodilation)
Anesthetic Considerations in Pulmonary Hypertension
Anesthesia in Primary/Secondary Pulmonary Hypertension and RV Failure
- Maintain chronic medication for pulmonary hypertension (Ca2+ antagonists, sildenafil, ET antagonists, i.v. PGI2)
- Intravenous PGI2 is switched to inhalation
- Mild premedication
- Insertion of PA catheter before induction (CVP, PA)
Anesthesia in Primary/Secondary Pulmonary Hypertension and RV Failure
- TIVA (propofol/opioid).
- Avoid ketamine, N2O (increases PVR) and inhalation agents (negative inotropic effect)
- TEE for monitoring RV function
- Hypoxia and hypercapnia increase PVR
- Regional anesthesia: undesirable drop in blood pressure and RV failure
- Noradrenaline for high SVR (MAP)
- Inhalation NO, prostacyclin and/or milrinone (selective reduction of PVR)
- In case of RV failure, i.v. milrinone + noradrenaline

Conclusions
- Noradrenaline + inhalation of vasodilators in pulmonary hypertension and RV failure
- The prevalence of chronic heart failure is continuously increasing
- Understand the pathophysiology
- Identify high-risk patient
- Anesthesia technique is less important
- Adequate monitoring
- Use inotropic/vasoactive drugs
- Do not forget the diagnosis of dynamic LV outflow obstruction in cases of sudden and severe intraoperative cardiogenic shock
Treatment of Heart Failure with Inotropic and Vasoactive Drugs
Chronic Heart Failure
- Prevalence ≈ 2%
- > 75 years, prevalence ≈ 10 %
- Within 10-20 years, the prevalence has increased 2-3 times
- Increased age
- Today, more people survive acute coronary syndromes

Inotropic Treatment
- Acute decompensation of chronic heart failure (ICM, DCM)
- Hypotension
- Hypoperfusion
- Acute coronary syndrome
- Extensive myocardial damage LV, RV
- VSD, papillary muscle rupture (MI)
- “Myocardial stunning” after revascularization
- Postoperative failure after heart surgery/transplantation
- Septic shock – septic cardiomyopathy
- Myocarditis
- Postpartum cardiomyopathy
- Right ventricular failure (pulmonary embolism, ARDS)


Inotropic Drugs
- Adrenaline
- Norepinephrine
- Isoprenaline
- Dopamine
- Dobutamine
- Phosphodiesterase inhibitors
- Milrinone
- Calcium sensitizers
- Levosimendan



Adrenaline (Epinephrine)
- Dose given in ng/kg/min
- 10-30 ng/kg/min: beta 1, 2-stimulation
- 30-100 ng/kg/min: alpha + beta-stimulation
- > 100 ng/kg/min: alpha-stimulation
- Tachycardia
- Vasoconstriction
- Arrhythmias
Noradrenaline (Norepinephrine)
- Beta-receptor stimulating effect similar to adrenaline
- Stimulates alpha-receptors at low concentrations
- Given in low SVR and hypotension
- Sepsis and “Systemic inflammatory response syndrome” (SIRS)
- Less tachycardia and arrhythmias compared to adrenaline
Isoprenaline
- Beta-1, 2 stimulation only
- Positive inotropic and chronotropic effect
- Vasodilation and hypotension
- Given in bradyarrhythmias and AV block
Dopamine
- Dose given in µg/kg/min
- 0.5-2.5 µg/kg/min: stimulates dopamine receptors
- 1-10 µg/kg/min: beta-receptor stimulation
- 5-10 µg/kg/min: alpha-stimulation
- Tachycardia, arrhythmias
- Decreases SVR at low doses
- Vasoconstriction, SVR, and PCWP increase with increasing doses
- Increased MVO2
- Good for heart failure and hypotension
Dobutamine
- Beta-1, 2 stimulation (d-dobutamine), SVR unchanged
- Alpha-stimulation (l-dobutamine), SVR unchanged
- At higher doses, beta-2 effect dominates over alpha, MVO2 unchanged/increased i.e., SVR and PCWP decrease
- Tachycardia, arrhythmias MVO2 unchanged/increased
- 2-15 µg/kg/min
Limiting Factors in the Use of Catecholamines
- Downregulation of beta and alpha receptors
- Tolerance development
- Tachycardia, arrhythmias
- Does not improve survival in LV failure
Phosphodiesterase Inhibitors (milrinone)


- Less significant increase in heart rate compared to dobutamine
- Better vaso-venodilation compared to dobutamine
- Additive effect to β stimulants
- Does not increase MVO2
- Less pronounced tachyphylaxis compared to β stimulants
Levosimendan


Levosimendan – Hemodynamics




Calcium Sensitizers and Diastole

Levosimendan and Diastolic Function in the Clinic
- Patients (n=23) with AVR due to aortic stenosis
- Randomized postoperatively to:
- placebo (n=11)
- levosimendan (0.1 and 0.2 µg/kg/min) (n=12)
- Left ventricular isovolumetric relaxation time (IVRT)
- Heart rate, filling pressure, arterial pressure were kept constant with pacing, colloid, and phenylephrine


Inotropic and Lusitropic Effects of Levosimendan vs. Milrinone
- Patients (n=31) with AVR due to aortic stenosis
- Randomized postoperatively to:
- milrinone 0.4 and 0.8 µg/kg/min (n=16)
- levosimendan 0.1 and 0.2 µg/kg/min (n=15)
- Strain echocardiography (TEE):
- LV strain (2-chamber, posterior wall)
- RV strain (4-chamber, free wall)
- Strain rate systole (SR-S)
- Strain rate early diastole (SR-E)
- Heart rate, filling pressure, arterial pressure were kept constant with pacing, colloid, and phenylephrine



Inotropic and Vasoactive Drugs in Cardiogenic Shock
“At present, there are no robust and convincing data to support a specific inotropic therapy as the best solution to reduce mortality in hemodynamically unstable patients with cardiogenic shock complicating AMI.” Cochrane Database Syst Rev. 2014 Jan 2;1:CD009669. doi: 10.1002/14651858.CD009669.pub

Dopamine or Noradrenaline as Vasopressor in Cardiogenic Shock?



Adrenaline or Noradrenaline?
- 57 patients with AMI + PCI and cardiogenic shock
- Randomized to
- adrenaline (n=27)
- noradrenaline (n=30)
- Target MAP 65-70 mmHg
- Primary end-point: change in cardiac output over 72 hours
- Safety end-point: refractory cardiogenic shock


Levosimendan vs Dobutamine in Cardiogenic Shock
- 22 patients with STEMI and PCI
- Cardiogenic shock
- Randomized to:
- levosimendan (n=11) 24 µg/kg + 0.1 µg/kg/min
- dobutamine (n=11) 5 µg/kg/min
- No IABP

Levosimendan vs Enoximone (Phosphodiesterase Inhibitor) in Cardiogenic Shock
- Cardiogenic shock after PCI due to AMI
- IABP
- norepinephrine (≈0.25 µg/kg/min)
- dobutamine (≈10 µg/kg/min)
- Randomized to:
- levosimendan (n=16)
- enoximone (n=16)
- End-point: 30-day mortality

Inotropic and Vasoactive Drugs in Right Ventricular Failure
Right Ventricular Failure (RVF)
Cardiac Causes
- Coronary artery disease (RV infarction)
- Valvular diseases
- Cardiomyopathy (ischemic, dilated)
- Heart surgery (CABG, AVR, MVR)
- Heart transplantation
- Post-LVAD
Extracardiac Causes
- Pulmonary embolism
- Lung diseases (COPD, ARDS)
- Primary pulmonary hypertension
- Sepsis
- Lung transplantation
- Post-thrombendarterectomy



Inhaled NO in RVF after Posterior AMI
- Thirteen patients with RV infarction and cardiogenic shock
- Inhalation of NO (80 ppm)

Inhaled NO in Heart Transplantation and RVF

Inhalation of Prostaglandins and Milrinone – Doses
- Prostacyclin (Flolan®): 10 µg/ml, 5-10 ml/h
- Iloprost (Ilomedin®, Ventavis®): 10 µg/ml, 2.5-5 µg x 6-9
- Treprostinil (Remodulin®): 30-50 µg x 4
- Milrinone: 1 mg/ml, 5-10 ml/h



Renal Effects of Inodilators
Cardiac output increase leads to increased RBF affecting GFR?




Renal Effects of Milrinone
- Patients undergoing cardiac surgery with normal preoperative renal function (n=27)
- Two groups:
- severe heart failure after weaning from CPB requiring milrinone (n=8)
- no heart failure after CPB (n=19)
- Systemic hemodynamics (PAC)
- Renal blood flow (RBF), renal vascular resistance (RVR), glomerular filtration rate (GFR), renal oxygen extraction (RO2Ex)
- Measurements: T0 =30’after CPB, T1=60’ after CPB


Renal Effects of Levosimendan?
”Effects of Levosimendan on Glomerular Filtration Rate, Renal Blood Flow, and Renal Oxygenation After Cardiac Surgery With Cardiopulmonary Bypass: A Randomized Placebo-Controlled Study”
Bragadottir et al Crit Care Med 2013;41:2328
- Uncomplicated cardiac surgery, normal renal function
- ICU, sedated, mechanically ventilated
- Randomized to:
- placebo, n=15
- levosimendan, n=15, 12µg/kg + 0.1 µg/kg/min
- Systemic hemodynamics (PAC)
- Renal blood flow (RBF), renal vascular resistance (RVR), glomerular filtration rate (GFR), renal oxygen consumption (RVO2), renal oxygen extraction (RO2Ex), filtration fraction



“Differential Effects of Levosimendan and Dobutamine on Glomerular Filtration Rate in Patients with Heart Failure and Renal Impairment: A Randomized Double-Blind Controlled Trial”
Lannemyr et al J Am Heart Assoc 2018;e008455
- Chronic heart failure (NYHA III-IV), LVEF < 40%
- Renal impairment: GFR < 80 ml/min
- Randomized to:
- dobutamine 7.5 µg/kg/min (n=16)
- levosimendan 12 µg/kg +0.1 µg/kg/min (n=16)
- Central hemodynamics
- Renal blood flow (RBF), GFR, renal oxygenation
- Renal vein catheter, infusions clearance of PAH and 51Cr-EDTA





Conclusions
- Inotropic treatment is indicated in heart failure associated with hypotension/hypoperfusion
- Milrinone and levosimendan have similar hemodynamic effects
- Milrinone and levosimendan are equipotent in inotropic and lusitropic effects on both LV and RV
- Norepinephrine is preferred over dopamine in cardiogenic shock
- Levosimendan is the only inotropic drug that increases GFR
Guidance in the treatment of chronic heart failure with reduced systolic left ventricular function
Pharmacological Treatment of Heart Failure
The treatment of chronic heart failure with reduced ejection fraction (HFrEF) aims to reduce symptoms, improve quality of life, decrease hospitalizations, and improve survival. The foundation of therapy consists of the so-called four-pillar treatment and should be initiated early unless contraindicated. Similar principles may also be applied in heart failure with mildly reduced ejection fraction (HFmrEF).
Foundational Therapy (“Green fields”)

The following drug classes are recommended as core treatment:
- ACE inhibitors (ACEi) or alternatively ARBs, with consideration of switching to ARNI in persistently symptomatic patients
- Beta-blockers (BB)
- Mineralocorticoid receptor antagonists (MRA)
- SGLT2 inhibitors
Therapy should be up-titrated to target doses according to guidelines and patient tolerance.
Individualized Treatment According to Clinical Presentation
Initial drug combinations and add-on therapy should be adapted to the patient’s clinical profile.
Ischemic Heart Disease
- Foundational therapy with beta-blocker + SGLT2 inhibitor
- Followed by addition of ACE inhibitor + MRA
Marked Congestion (Volume Overload)
- SGLT2 inhibitor + ACE inhibitor
- Add MRA as needed
- Loop diuretics are used in cases of fluid retention
Impaired Renal Function
- SGLT2 inhibitor + beta-blocker
- Careful initiation and monitoring of ACE inhibitor and MRA
Hypotension
- Start with SGLT2 inhibitor
- Gradual addition of beta-blocker, ACE inhibitor, and MRA depending on tolerance
Hypertension
- ACE inhibitor + beta-blocker
- Followed by addition of SGLT2 inhibitor + MRA
Atrial Fibrillation (Normofrequent)
- SGLT2 inhibitor + ACE inhibitor
- Followed by beta-blocker + MRA
High Heart Rate (Sinus Rhythm)
- Beta-blocker + SGLT2 inhibitor
- Add ACE inhibitor + MRA as needed
- Ivabradine may be considered in patients with persistently elevated heart rate despite optimal beta-blocker therapy
Management of Persistent Symptomatic Heart Failure
If symptoms persist despite optimal foundational therapy, additional measures may be considered:
- Switch from ACE inhibitor/ARB to ARNI
- CRT-P or CRT-D in patients with wide QRS complexes
- ICD according to established indications
- Ivabradine in sinus rhythm with elevated heart rate
- Digoxin, particularly in rapid atrial fibrillation
- Nitrates when indicated
- Valve intervention in significant valvular disease
- Atrial fibrillation ablation
- Revascularization in ischemic etiology
- In advanced cases: heart transplantation or mechanical circulatory support (ventricular assist device)
Additional Important Measures
- Intravenous iron in cases of iron deficiency
- Lifestyle interventions (smoking cessation, physical activity, sodium restriction, weight control)
- Careful monitoring of blood pressure, renal function, and electrolytes
- Patient education and self-monitoring
In summary, modern heart failure management is based on early and combined initiation of multiple disease-modifying therapies, individualized according to hemodynamic status, heart rhythm, renal function, and comorbidities.
Antiarrhythmic Drugs – Vaughan Williams Classification
Antiarrhythmic drugs are categorized according to the Vaughan Williams classification, based on their primary effects on cardiac action potentials and ion channels.
The cardiac action potential (in working myocardium) consists of the following phases:
- Phase 0 – Rapid depolarization (Na⁺ influx)
- Phase 1 – Initial repolarization (K⁺/Cl⁻ efflux)
- Phase 2 – Plateau phase (Ca²⁺ influx)
- Phase 3 – Repolarization (K⁺ efflux)
- Phase 4 – Resting membrane potential
Class I – Sodium Channel Blockers (Na⁺)
Block fast sodium channels and primarily affect Phase 0 (depolarization rate).
Divided into three subclasses:
Class IA
- Procainamide
- Quinidine
- Disopyramide
→ Moderate sodium channel blockade
→ Prolong action potential duration (also some potassium channel blockade)
Class IB
- Lidocaine
- Mexiletine
→ Weak sodium channel blockade
→ Shorten action potential duration
→ Particularly effective for ventricular arrhythmias
Class IC
- Flecainide
- Propafenone
- Moricizine
→ Strong sodium channel blockade
→ Markedly slow conduction velocity
→ Minimal effect on action potential duration
Class II – Beta Blockers
- Propranolol
- Esmolol
Block β-adrenergic receptors and reduce sympathetic stimulation.
Effects:
- Decrease automaticity (Phase 4)
- Reduce sinus rate
- Slow AV nodal conduction
- Decrease risk of stress- or catecholamine-induced arrhythmias
Class III – Potassium Channel Blockers (K⁺)
- Amiodarone
- Dronedarone
- Dofetilide
- Sotalol
- Ibutilide
- Vernakalant
Primarily block potassium channels and prolong Phase 3 (repolarization).
Effects:
- Prolong action potential duration
- Prolong refractory period
- QT interval prolongation
Class IV – Calcium Channel Blockers (Ca²⁺)
- Verapamil
- Diltiazem
Block L-type calcium channels and primarily affect Phase 2 and AV nodal conduction.
Effects:
- Slow AV nodal conduction
- Reduce heart rate
- Used particularly in supraventricular tachycardias
Summary: Drug Class and Action Potential Phase
- Na⁺ influx (Phase 0) → Class I
- Ca²⁺ influx (Phase 2, nodal conduction) → Class IV
- K⁺ efflux (Phase 3) → Class III
- Automaticity (Phase 4) → Class II
Adrenaline (Epinephrine)
Adrenaline is a sympathomimetic catecholamine. The positive inotropic effect is primarily due to the agonistic effect on the heart’s beta1 receptors, but also on the heart’s alpha1 receptors.
Concentration: Common strength is 0.05 mg/ml or 0.1 mg/ml for continuous infusion. For manual injection, 0.1 mg/ml or lower strength 0.01 mg/ml.
Receptor Activity: α1 ++++, β1 ++++, β2 +++
Physiological Effects: SVR↑, CO↑, HR↑, BP↑, bronchodilation
Indication: Circulatory shock, refractory hypotension, allergic shock, anaphylaxis, cardiac arrest, severe heart failure, cardiogenic shock, severe poisoning, severe bronchospasm, status asthmaticus, severe stridor.
Dosage: 0.05-0.1-(0.30) μg/kg/min = 3-40 ml/h for 70 kg. Common starting dose is 0.1 μg/kg/min, adjusted according to blood pressure. Anaphylaxis/asthma: 0.3-0.5 mg IM, CPR 1 mg IV. For established circulation but severe heart failure, 0.1 mg IV in steps. For circulatory collapse, 0.1-1.0 mg IV, titrated according to blood pressure, avoid overdose.
Dosage Activity: <0.05 μg/kg/min – usually moderate effect on blood pressure, 0.05-0.1 μg/kg/min β1 effect, increased cardiac output, >0.1 μg/kg/min – α1 effect
Side Effects: Tachycardia, arrhythmias, uncontrolled blood pressure elevation.
Argipressin
Argipressin is a synthetic analog of pitressin. Argipressin induces systemic vasoconstriction, thereby increasing peripheral vascular tone with elevated blood pressure. It can also be administered locally to reduce bleeding during laparoscopic surgery for ectopic pregnancy or myomectomy.
Indication: Severe hypotension due to vasoplegia (refractory hypotension). Treatment failure with other inotropic drugs in low peripheral vascular resistance.
Dosage: 2.4-4.8 E/hour (which typically equates to 6-12 ml/h)
Concentration: 20 E/ml. Argipressin is diluted by mixing 1 ml of 1 ampule (1 ml = 20 E) with 49 ml of Glucose 5% in a 50-ml syringe, giving a concentration of 0.4 E/ml.
Side Effects: Headache, flushing, hypotension, pain in extremities, peripheral edema, blurred vision, nasal congestion, night sweats.
Warning: Caution in – angina pectoris, heart failure, renal failure, poorly controlled hypertension, anaphylaxis, or vasopressin hypersensitivity.
Dobutamine (Dobutamine Hameln®)
Positive inotropic drug with a mild vasodilatory effect. Dobutamine is a synthetic, sympathomimetic amine. The positive inotropic effect is primarily due to the agonistic effect on the heart’s beta1-receptors, but also on the heart’s alpha1-receptors.
Concentration: Standard solution 2 mg/ml.
Receptor Activity: α1 +, β1 ++++, β2 ++, DA-1 0.
Physiological Effects: SVR↓, CO↑, HR↑, BP+/-. Binds to and stimulates beta1 receptors in the heart. Increases contraction strength.
Indication: Low cardiac output, heart failure, sepsis.
Dosage: Recommended starting dose is 5 μg/kg/min, titrated to 2-20 μg/kg/min = 5-40 ml/h for 70 kg.
Dosage Activity: < 3 μg/kg/min – usually no effect on blood pressure or blood pressure drop, 5-10 μg/kg/min β1-effect, increased cardiac output, >10 μg/kg/min – α1-effect. Increased heart rate.
Side Effects: Tachycardia, blood pressure drop in hypovolemia.
Dopamine (Giludop®)
Dopamine is a sympathomimetic catecholamine. The positive inotropic effect is primarily due to the agonistic effect on the heart’s beta1-receptors, but also on the heart’s alpha1-receptors. Significant chronotropic effect.
Concentration: Standard solution 2 mg/ml
Receptor Activity: α1 ++, β1 ++++, β2 ++, DA-1 +++
Indication: Refractory hypotension, low cardiac output, heart failure, oliguria, sepsis.
Dosage: 3-15 μg/kg/min = 7-40 ml/h for 70 kg.
Dosage Activity: < 3 μg/kg/min – DA-effect, 5-10 μg/kg/min β1-effect, increased heart rate, > 10 μg/kg/min – α1-effect.
Side Effects: Tachycardia, arrhythmias, renal intestinal hypoperfusion, psychological symptoms, pituitary dysfunction.
Ephedrine
Ephedrine is a naturally occurring alkaloid. Ephedrine raises blood pressure by stimulating adrenergic alpha- and beta-receptors. Ephedrine acts directly on receptors but primarily works by releasing endogenous norepinephrine, which in turn affects the receptors. The positive inotropic effect primarily stems from its agonistic effect on the heart’s beta1 receptors, with some effect on the heart’s alpha1 receptors.
Receptor activity: α1 +, β1 +++, β2 ++, DA-1 0.
Physiological effects: Mildly increases inotropy, chronotropy, and blood pressure. Releases norepinephrine. Increased cardiac output (CO), increased blood pressure and mean arterial pressure. Increased SVR, reduced CO, increased HR, and increased BP. Short duration of effect (5-15 minutes) with intravenous administration. Slightly longer effect with subcutaneous or intramuscular administration.
Indications: Temporary blood pressure drop, vasodilation, bradycardia, blood pressure drop after spinal or epidural anesthesia, blood pressure drop post-anesthesia induction, bronchial asthma.
Side effects: Tachycardia, extrasystoles, arrhythmias, atrial fibrillation, myocardial ischemia.
Concentration: Solution 50 mg/ml. Common strength is 5 mg/ml (diluted) or 50 mg/ml.
Dosage: 5-10 mg intravenously. Typical starting dose is 5 mg intravenously, adjusted based on blood pressure and pulse. 25-50 mg can be given intramuscularly. Intramuscular doses may be administered concurrently with intravenous doses, for example, 5 mg IV plus 25 mg intramuscularly during spinal anesthesia.
Dosage activity: 5-10 mg usually results in a moderate effect on blood pressure, with unchanged CO; > 10 mg also increases CO.
Levosimendan (Simdax®)
Levosimendan increases the calcium sensitivity of contractile proteins through calcium-dependent binding to cardiac troponin C. Additionally, it opens ATP-sensitive potassium channels in vascular smooth muscle, leading to vasodilation of systemic and coronary resistance vessels and systemic venous capacitance vessels.
Receptor activity: Calcium sensitizer.
Concentration: Solution 2.5 mg/ml. Common strength is 0.025 or 0.05 mg/ml.
Physiological effects: Increased contractility, CO↑, HR↑, vasodilation, increased ejection fraction, decreased SVR, lowered blood pressure.
Indications: Circulatory shock, severe heart failure, cardiogenic shock, “stunned myocardium.”
Dosage: 6-12 μg/kg/min for 10 minutes followed by continuous infusion at 0.1 μg/kg/min for 24 hours. Common starting dose is 6 μg/kg/min, adjusted based on blood pressure.
Dosage activity: 0.05-2 μg/kg/min typically has moderate effects on blood pressure, causing hypotension.
Contraindications: Severe hypotension, hypokalemia, hypovolemia, tachycardia, mechanical obstruction of the left ventricle, Torsades de Pointes arrhythmia, renal impairment.
Side effects: Tachycardia, hypotension, headache, atrial fibrillation, ventricular extrasystoles, arrhythmias, hypokalemia.
Phenylephrine
Phenylephrine is a sympathomimetic substituted phenethylamine. Pure alpha-agonist. Causes vasoconstriction and increases blood pressure. Reduced cardiac output (CO), increased diastolic blood pressure, and mean arterial pressure (MAP).
Receptor activity: α1 +++, β1 none, β2 none, DA-1 none.
Physiological effects: Increased SVR, reduced CO, reduced HR, increased BP, reflex bradycardia.
Indications: Hypotension, vasodilation, blood pressure drop after spinal or epidural anesthesia.
Side effects: Bradycardia, heart failure, pulmonary edema.
Concentration: Ready-made solution 0.1 mg/ml. Common strength is 0.1 mg/ml, also available at 10 mg/ml.
Dosage: 0.1-0.2 mg IV. Typical starting dose is 0.1 mg IV, adjusted based on blood pressure. Phenylephrine is often given in repeated boluses but can also be administered as a continuous infusion at 0.1 mg/ml. Typical dosage is 0.05-0.5 μg/kg/min = approximately 3-20 ml/h for 70 kg.
Dosage activity: < 0.3 mg usually results in a moderate effect on blood pressure with unchanged CO; > 0.5 mg reduces CO and causes vasoconstriction.
Milrinone (Corotrop®)
Milrinone is a bipyridine derivative with both positive inotropic and vasodilating effects, but with minimal chronotropic effects.
Receptor activity: Phosphodiesterase-III inhibitor.
Physiological effects: SVR↓, CO↑, HR↑, BP+/-. Increases cardiac contractility and stroke volume, acts as a vasodilator.
Indications: Severe heart failure, cardiogenic shock.
Concentration: Solution 1 mg/ml. Common strength for continuous infusion is 0.1 mg/ml (100 µg/ml) or 0.15 mg/ml (150 µg/ml).
Dosage: Initially, a slow (10 minutes) intravenous injection of 50 µg/kg, followed by continuous infusion at 0.37-0.75 μg/kg/min. Common starting dose is 0.5 μg/kg/min, adjusted based on blood pressure. Most patients see hemodynamic improvement within 5-15 minutes. Doses in the range of 0.375-0.50 µg/kg/min tend to maximize the initial increase in cardiac output, while doses in the range of 0.50-0.75 µg/kg/min tend to optimize improvements in pre- and afterload parameters such as PCW pressure (pulmonary capillary wedge), MAP, and SVR.
Dosage activity: < 0.375 μg/kg/min typically results in moderate effects on circulation, 0.5-0.75 μg/kg/min beta1 effect, increase in BP, CO, and EF.
Contraindications: Hypovolemia, obstructive aortic or pulmonary valve defects. Caution should be exercised during acute myocardial infarction.
Side effects: Hypotension, increased myocardial oxygen consumption, tachycardia, VES, VT.
Isoprenaline
Isoprenaline is a sympathomimetic amine. The positive inotropic effect is primarily due to its agonistic effect on the heart’s beta1-receptors and beta2-receptors, with some effect on the heart’s alpha1-receptors. Isoprenaline is vasodilatory with a pronounced positive chronotropic effect.
Concentration: Common strength 0.2 mg/ml.
Receptor activity: α1 none, β1++++, β2 ++++, DA-1 none. Positive chronotropic and inotropic effects on the heart. Potent vasodilation and increased heart rate. Increased cardiac output (CO), reduced diastolic blood pressure, and mean arterial pressure.
Physiological effects: Decreased SVR, CO↑↑, HR↑↑, decreased BP, bronchodilation.
Indications: Circulatory shock, bradycardia, AV-block III, refractory hypotension, cardiac arrest, severe heart failure with low CO, cardiogenic shock, certain severe poisonings.
Dosage: 0.01-0.15 μg/kg/min, 15-30 ml/h for 70 kg. Typical starting dose is 0.05 μg/kg/min, adjusted based on blood pressure.
Dosage activity: < 0.05 μg/kg/min – generally moderate effect on blood pressure, possible BP drop, increased CO; 0.05-0.1 μg/kg/min β1-effect, increased cardiac output, increased heart rate.
Side effects: Tachycardia, blood pressure drop, arrhythmias.
Nitroglycerin
Nitroglycerin is a prodrug that is converted into nitric oxide (NO). Nitric oxide causes relaxation of vascular smooth muscle by increasing cyclic guanosine monophosphate (cGMP). The vasodilatory effect is predominantly venous, but arterial dilation also occurs (venous > arterial).
Mechanism of Action
- Nitroglycerin is metabolized to nitric oxide (NO) in smooth muscle.
- NO activates guanylate cyclase.
- Guanylate cyclase converts GTP into cGMP.
- Increased cGMP inhibits the Ca²⁺–calmodulin complex.
- This decreases myosin light chain kinase (MLCK) activity.
- Reduced MLCK activity decreases actin–myosin cross-bridge formation.
- The result is smooth muscle relaxation and vasodilation.
Dosage:
Continuous infusion: 1–5 mL/hour, corresponding to 20–80 μg/min or 0.1–1.6 μg/kg/min.
Initial dose: 0.5 μg/kg/min.
Hemodynamic Effects
Venous dilation
→ Decreased venous return
→ Reduced preload
Arterial dilation
→ Reduced systemic vascular resistance (SVR)
→ Reduced afterload
Overall effects:
- ↓ Systemic vascular resistance (SVR)
- ↓ Pulmonary vascular resistance (PVR)
- ↓ Preload
- ↓ Myocardial oxygen demand
Clinical Implications
- Reduces myocardial wall stress
- Improves subendocardial perfusion
- Used in angina, acute coronary syndromes, pulmonary edema, and perioperative hypertension
Nitroglycerin also dilates both normal and stenotic coronary arteries.
Comparison with Nitroprusside
- Nitroprusside dilates arterial and venous vessels equally.
- Nitroglycerin predominantly dilates venous vessels (venous > arterial).
Norepinephrine
Norepinephrine is a sympathomimetic amine. The positive inotropic effect is primarily due to its agonistic effect on the heart’s beta1-receptors, but also on its alpha1-receptors.
Concentration: Common strength for continuous infusion is 0.1 mg/ml. “Double strength” is 0.2 mg/ml. Weak strength is 0.05 mg/ml.
Receptor activity: α1 +++, β1 +++, β2 +. DA-1 none.
Physiological effects: SVR↑, CO+/-, HR↑, BP↑↑.
Indications: Circulatory shock, refractory hypotension, sepsis, anaphylaxis, severe hypotension with vasodilation, cardiogenic shock, severe poisonings.
Side effects: Tachycardia, arrhythmias, renal intestinal hypoperfusion, peripheral ischemia, bowel ischemia, splanchnic ischemia.
Dosage: 0.01-0.1-(0.5) μg/kg/min = 3-40 ml/h for 70 kg. Typical starting dose is 0.05 μg/kg/min, adjusted based on blood pressure.
Dosage activity: < 0.05 μg/kg/min – generally moderate effect on blood pressure, 0.05-0.1 μg/kg/min β1-effect, blood pressure increase; > 0.1 μg/kg/min α1-effect, significant blood pressure increase, vasoconstriction, tachycardia.
Contraindications: Hypertension, hypovolemia, hyperthyroidism, peripheral hypoxia, peripheral vasoconstriction, hyperadrenergic states.
Vasopressin
Vasopressin is an antidiuretic hormone that regulates water reabsorption in the kidney’s distal tubules. It regulates water balance and increases urine osmolarity, leading to increased peripheral vasoconstriction and elevated blood pressure.
Receptor activity: V2 +++, α1 none, β1 none, β2 none, DA-1 none.
Physiological effects: SVR↑↑, CO↓, HR↓, BP↑↑.
Indications: Sepsis, adjunct treatment to vasopressor therapy with norepinephrine in septic shock.
Side effects: Bradycardia, vasoconstriction, pulmonary edema, arrhythmias, renal intestinal hypoperfusion, peripheral ischemia, bowel ischemia.
Concentration: Common strength is 0.4 IU/ml.
Dosage: 0.01-0.06 IU/min = 2-4 ml/h for 70 kg. Typical starting dose is 0.04 IU/min, adjusted based on blood pressure. Higher doses are used for hemorrhagic shock than for sepsis treatment.
Dosage activity: < 0.02 IU/min causes a slight increase in blood pressure, > 0.04 IU/min – α1-effect, significant blood pressure increase, vasoconstriction.
Contraindications: Hypertension, hypovolemia, hyperthyroidism, peripheral hypoxia, peripheral vasoconstriction, hyperadrenergic states.
Cordarone (Amiodarone)
Antiarrhythmic. Prolongs the action potential phase 3 in cardiac fibers by inhibiting potassium channels. Reduces sinus automaticity, leading to a lower heart rate. Exhibits non-competitive alpha- and beta-blockade.
Dosage: 5 mg/kg body weight administered via intravenous infusion over a period of 20 minutes to 2 hours as slowly as possible, depending on the clinical situation. This amount is given as a diluted solution in 250 ml of glucose 50 mg/ml. Typically, 300 mg is given over 30 minutes, followed by an additional 900-1200 mg over 24 hours, with the infusion rate adjusted based on the clinical response. In resuscitation, Cordarone can be given as a bolus dose of 300 mg in 20 ml of glucose.
Indications: Severe symptomatic ventricular and supraventricular arrhythmias, including atrial flutter/fibrillation.
Concentration: Injection solution 50 mg/ml. Common strength 50 mg/ml.
Side effects: Bradycardia, hypotension, corneal microdeposits, hypothyroidism.
Warning: Very rare cases of interstitial pneumonitis have been reported with intravenous amiodarone.
Here is the translation you requested, keeping the original structure intact:
—
Corotrop (Milrinone)
Milrinone is an inotropic drug that acts as a phosphodiesterase III inhibitor.
Physiological effects: SVR↓, CO↑, HR↑, BP+/-. Increases contractility and stroke volume. Vasodilator.
Dosage: Initially, a slow (10-minute) intravenous injection of 50 µg/kg, followed by continuous infusion at 0.37-0.75 µg/kg/min. The usual starting dose is 0.5 µg/kg/min, adjusted based on blood pressure. Hemodynamic improvement is usually observed within 5-15 minutes in the majority of patients. Doses in the range of 0.375-0.50 µg/kg/min tend to maximize the initial improvement in cardiac output, while doses in the range of 0.50-0.75 µg/kg/min tend to optimize improvements in pre- and afterload parameters such as PCW pressure, MAP, and SVR.
Dosage activity: <0.375 µg/kg/min – generally moderate effect on circulation; 0.5-0.75 µg/kg/min β1-effect, increased BP, CO, and EF.
Indications: Severe heart failure, cardiogenic shock.
Concentration: Solution 1 mg/ml. Common strengths: 0.2 mg/ml or 100 µg/ml or 150 µg/ml.
Side effects: Hypotension, increased myocardial oxygen consumption, tachycardia, ventricular extrasystoles, ventricular tachycardia.
Contraindications: Hypovolemia, obstructive aortic or pulmonary valve defect. Exercise caution in cases of acute myocardial infarction.
Simdax (Levosimendan)
Calcium sensitizer with positive inotropic effect.
Physiological effects: Increases cardiac contractility, CO↑, HR↑, vasodilation, increased ejection fraction, blood pressure reduction, reduced SVR. Levosimendan increases contractility and reduces both preload and afterload without negatively affecting diastolic function. It also activates “stunned” myocardium.
Dosage: 6-12 µg/kg/min for 10 minutes, followed by continuous infusion at 0.1 µg/kg/min for 24 hours. The usual starting dose is 6 µg/kg/min, adjusted based on blood pressure. Avoid bolus doses in cases of risk for blood pressure drops.
Indications: Short-term treatment of acute decompensated chronic heart failure (ADHF) when conventional treatment is inadequate, and inotropic support is considered appropriate.
Concentration: Solution 2.5 mg/ml, common strengths: 0.025 mg/ml or 0.05 mg/ml.
Side effects: Tachycardia, blood pressure drop, headache, atrial fibrillation, ventricular arrhythmias, hypokalemia.
Dosage activity: 0.05-2 µg/kg/min – generally moderate effect on blood pressure, blood pressure drop.
Contraindications: Severe hypotension and tachycardia, mechanical obstruction of the left ventricle, Torsade de Pointes, severely impaired renal function. Correct hypokalemia and hypovolemia.
Remodulin (Treprostinil)
Treprostinil is a prostacyclin analogue. The primary pharmacological effects of prostacyclin (PGI2) include marked vasodilation of the pulmonary and systemic circulation, inhibition of platelet aggregation, and antiproliferative effects. It directly exerts a vasodilatory effect on the pulmonary and systemic circulation and inhibits platelet aggregation.
In animal studies, this vasodilatory effect reduces afterload in both the left and right ventricles, while increasing cardiac output and stroke volume. The effect of treprostinil on heart rate is dose-dependent. No significant effects have been observed on AV conduction.
Dosage: The recommended initial infusion rate is 1.25 ng/kg/min. If the initial dose is not well tolerated, the infusion rate can be reduced to 0.625 ng/kg/min. The infusion rate should be gradually increased under medical supervision by 1.25 ng/kg/min per week for the first four weeks of treatment, and then by 2.5 ng/kg/min per week.
Indications: Pulmonary hypertension, right ventricular failure.
Concentration: Each ml contains 1 mg, 2.5 mg, 5 mg, or 10 mg treprostinil as treprostinil sodium. Administered as an intravenous infusion via a central line.
Side effects: Blood pressure drop, vasodilation, prolonged bleeding time, jaw pain, headache, leg pain, diarrhea, nausea. All are dose-dependent.
Warning: Side effects include chest rigidity, breathing difficulties, irregular heart rhythm, skin hemorrhages, hematuria.
Ventavis (Iloprost)
A synthetic prostacyclin analogue that is inhaled via a nebulizer. Provides selective reduction of vascular resistance in the pulmonary circulation.
Indication: Primary pulmonary hypertension (PPH).
Dosage: 2.5-5 micrograms per dose x 6-9/day. At the start of treatment with iloprost, the first inhaled dose should be 2.5 micrograms of iloprost delivered through the nebulizer’s mouthpiece. If the dose is well tolerated, it should be increased to 5 micrograms of iloprost and maintained at that level. If the 5-microgram dose is poorly tolerated, it should be reduced to 2.5 micrograms.
Concentration: Nebulizer solution 20 micrograms/ml.
Side effects: Bleeding, thrombocytopenia, headache, vasodilation, flushing, chest pain, cough, peripheral edema.
Warning: The vasodilatory effect in the lungs following inhalation of iloprost has a short duration (1-2 hours). Blood pressure should be monitored before initiating Ventavis treatment. For patients with low systemic blood pressure or those receiving medications that lower blood pressure, caution should be exercised to avoid further hypotension. Ventavis treatment should not be started in patients with systolic blood pressure under 85 mmHg.
