Author:
Kai Knudsen
Updated:
20 March, 2026
Here, severe and life-threatening infections such as sepsis and septic shock are described, including diagnosis and appropriate treatment. The selection of relevant antibiotic therapy for different types of infections, including choice of drugs and correct dosing, is covered. The sensitivity of bacteria to various antibiotics and the different mechanisms of action of antibiotics are also described.
- Life-threatening Infections
- Duration of antibiotic therapy for common infections
- Classification of bacteria
- Classification of antibiotics
- Sepsis and Septic Shock
- Sepsis risk stratification
- Sepsis Recognition — 2025 Practical Guide
- Sepsis Alarm
- Antibiotic Treatment in the Intensive Care Unit
- Antibiotic Choice in Severe Sepsis
- Bacterial Sensitivity to Various Antibiotics
- Antibiotics for Reduced Renal Function
- Parenteral Antibiotics for Children
- Fungal Infections in Intensive Care
Life-threatening Infections
Sepsis and other severe infections mean that a serious infection affects the entire body, causing damage to vital organs such as the heart, lungs, brain, and kidneys, which may stop functioning properly. Sometimes, even a mild infection can quickly develop into a critical condition that leads to multi-organ failure. The affected person often feels very ill and finds it difficult to manage independently. Symptoms often appear suddenly, sometimes within a few hours. In relevant cases, investigation and identification of the infection focus with surgical intervention (incision, drainage, excision, amputation, debridement, decompression, etc.) when possible are done promptly, striving for “Source control” along with appropriate antibiotic treatment. Antibiotic therapy is the cornerstone of treating severe infections, a common condition among ICU patients. Collecting relevant cultures (respiratory secretions, wound culture, urine culture, blood cultures, CSF) before antibiotic treatment is crucial but should not delay the initiation of antibiotics in life-threatening infections. In septic shock, always administer an extra loading dose of β-lactam antibiotics (cefotaxime, pip/taz, or meropenem) approximately 3 hours after the first dose. Serious and complicated infections should be evaluated by an infectious diseases consultant within 24 hours or no later than the next business day.

Addition of aminoglycoside (AG) should be considered in septic shock if the infection is suspected to be caused by G-neg bacteria (unknown focus, urosepsis, abdominal infection) and other β-lactam antibiotics than meropenem are being used.
Contraindications for aminoglycosides: chronic/(acute) renal failure, hearing impairment. Tobramycin (Nebcina©) is dosed at 7 mg/kg x 1. For increased risk of ESBL bacteria (previous ESBL infection, care/stay in ESBL-endemic countries in the last 3 months), amikacin (ESBL bacteria often resistant to tobramycin) is given instead. Amikacin (Biklin©) is dosed at 25 mg/kg x 1. If BMI >30, AG is dosed based on “adjusted body weight” (ABW) according to the formula: ABW = IBW + 0.4 x (TBW-IBW). Usually, one dose of AG is sufficient, but further dosing is guided by concentration determination after 24 hours (trough level).
Additional treatment with vancomycin should be considered for known MRSA carriage (not for urinary focus) and suspected CVL-related coagulase-negative staphylococci infection. Loading dose: 30 mg/kg (max 2 g), followed by 15 mg/kg x 3 (lower dose in established renal failure – consult infectious diseases). Trough level determination before the 4th dose. Vancomycin can also be administered as a continuous infusion.
Echinocandin (caspofungin, micafungin, anidulafungin) should be considered in the presence of risk factors for invasive fungal infection.
Renal failure/dialysis: Give the initial dose of β-lactam antibiotics, as well as an extra loading dose (3 hours) in septic shock, as with normal kidney function.
Common Severe Infections:
- Abdominal infections
- Intestinal infections
- CNS infections
- Endocarditis
- Gynecological infections
- Skin and soft tissue infections
- Joint and bone infections
- Lower respiratory tract infections (influenza, Covid-19, pneumonia, COPD exacerbations, chronic bronchitis)
- Neutropenic fever
- Suspected infection without sepsis/septic shock
- Sepsis and septic shock
- STIs (rarely cause systemic symptoms)
- Urinary tract infections (cystitis, pyelonephritis, pyelitis)
- Thoracic abscesses
Common Symptoms of Severe Infections:
- Fever
- Chills
- Difficulty breathing, dyspnea, tachypnea
- Confusion, altered consciousness, somnolence
- Diarrhea or vomiting
- Severe abdominal pain, or pain in the back, muscles, or joints
- Muscle weakness (especially in older individuals)
- Possible localized swelling, redness, and pain in soft tissue infections
Not all symptoms may be present, but the more symptoms, the higher the likelihood of sepsis. Fever is common, but not everyone will have it.
Investigation and Diagnostics of Severe Infections
| Source | Unknown focus | Pneumonia | Abdominal infection | Acute bacterial meningitis |
|---|---|---|---|---|
| Cultivation of: | • Peripheral blood • CVC + arterial blood • Urine/wound/saliva | • Peripheral blood • CVC + arterial blood • Tracheal mucosa/ saliva/NPH | • Peripheral blood • CVC + arterial blood | • Peripheral blood • CSF |
| Other microbiological diagnostics | • Betaglucan [risk of invasive candida: prolonged ICU care (> 10 days), neutropenia, intestinal perforation, CVVHD] as needed | • U-antigen pneumoc + Legionella • Airway block (virus-PCR) • Atypical bacterias (PCR) • TB-diagnostics • Pneumocystis-PCR + β-glukan as needed | • Betaglucan [risk of invasive candida: prolonged ICU care (> 10 days), neutropenia, intestinal perforation, CVVHD] as needed | • CSF-PCR (bacterieas) • HSV-1 PCR (diff - diagnosis herpes encephalitis) |
Initial Antibiotic Treatment in Severe Infections
| Source | Unknown Foci3 | Pneumonia3 | Abdominal Infection | Acute bacterial meningitis |
|---|---|---|---|---|
| Community Acquired Infection | a. Pip/Taz 4g x 3-41 b. Cefotaxime 2g x 3 c. Meropenem 1g x 3-41 +/- aminoglycoside2 | a. Cefotaxime 2g x 3 + Erythromycin 1g x 3 b. Phenoxymethyl-PcV 3g x 4 + Moxifloxacine 400mg x 1 | a. Pip/Taz 4g x 3-41 b. Cefotaxime 2g x 3 + Metronidazol 1,5g x 1 c. Meropenem 1g x 3-41 +/- Aminoglycoside2 | Meropenem 2g x 3 + Betametason 8mg x 4 |
| Nosocomial Infection (>48 hours. after arrival to hospital) | a. Pip/Taz 4g x 3-41 b. Meropenem 1g x 3-41 +/- Vancomycin3 +/- Aminoglycoside2 | a. Pip/Taz 4g x 3-41 b. Meropenem 1g x 3-41 +/- Aminoglycoside2 | a. Pip/Taz 4g x 3-41 b. Meropenem 1g x 3-41 +/- Aminoglycoside2 | Meropenem 2g x 3 + Vancomycin 15mg/kg x 3 |
| Neutropenia (neutrofiles ≤ 0,5) | a. Meropenem 1g x 4 b. Pip/Taz 4g x 4 +/- Aminoglycoside2 | a. Pip/Taz 4g x 4 + Moxifloxacine 400 mg x 1 b. Meropenem 1g x 4 + Moxifloxacine 400mg x 1 | a. Meropenem 1g x 4 b. Pip/Taz 4g x 4 +/- Aminoglycoside2 | Meropenem 2g x 3 + Betametason 8mg x 4 |
| Severe allergy against beta-lactam antibiotics (anaphylactic shock, swelling/obstruction of respiratory tract) | Clindamycin 600 mg x 3-4 + Ciprofloxacin 400 mg x 3 +/- Aminoglycoside2 | a. Clindamycin 600 mg x 3-4 + Moxifloxacine 400 mg x 1 b. Clindamycin 600 mg x 3-4 + Ciprofloxacin 400 mg x 3 (at hospitalized infection/suspicion of pseudomonas) | Clindamycin 600 mg x 3-4 + Ciprofloxacin 400 mg x 3 +/- Aminoglycoside2 | a. Meropenem 2g x 3 (not in the case of shock due to beta-lactam antibiotics) b. Moxifloxacin + Vancomycin 15mg/kg x 3 + Trim/Sulphoxazine 20 ml x 2 (in the case of shock due to beta-lactam antibiotics) |
| Please consider carefully | • Rec. for "Unknown focus" includes urinary focus • Necrotising soft tissue infection (Fasciitis): Meropenem 1g x 4 + Clindamycin 600 mg x 3-4 + possible. iv immunoglobuline (GAS/S. aureus) • Endocarditis in cardiac valve disease or heart murmurs • Malaria: Africa/Asia | • Legionella: international travel, immunosuppression, chronic lung disease • Pneumocystis/aspergillus: immunosuppression • Tuberculosis: origin, age, immunosuppression, addiction, long-term progression • Influenza: Oseltamivir (Tamiflu®) 75 mg x 2 p.o. + Cefotaxime 2 g x 3 | • Early "source control" • Invasive candida: prolonged ICU care, neutropenia, intestinal perforation, CVVHD Fluconazole i.v. 800 mg x 1 day 1, then 400 mg x 1, at sepsis Micafungine 100 mg x 1 | • TB meningitis: descent • Fungal meningitis: immune suppression • Herpes encephalitis: focal symptom Acyclovir 10 mg/kg x 3 |
| Serious and complicated infections should be assessed by infection consultant/back-up within 24 hours or no later than next weekday. | ||||
| 1Betalactam antibiotics: As a result of increased volume of distribution, high and frequent doses should always be given (Pip/Taz 4g x 4, Cefotaxime 2g x 3, meropenem 1g x 4). In addition, provide an additional loading dose of selected beta-lactam antibiotic approximately 3 hours after the first dose. As the condition stabilizes, the usual dose of beta-lactam antibiotics should generally be given. | ||||
| 2Supplementary therapy with aminoglycoside should always be considered during sepsis and septic shock (Sepsis-3) if the infection can be caused by gram-negative bacteria (unknown focus, urosepsis, abdominal infection, VAP). Tobramycin (Nebcin©) is given at a dose of 7 mg/kg x 1. In case of obesity, the dose should be based on estimated ideal body weight. In case of increased risk of ESBL bacteria (ESBL infection, overseas care, stay in an ESBL endemic country last 6 months or treatment with cephalosporines/kinolones last 3 months) instead, amicacine is given because ESBL bacteria are often resistant to tobramycine too. Amicacin (Biklin©) is given in the dose of 25 mg/kg x 1 with dose adjustment in obese patients as above. Often enough a dose of aminoglycoside but any continued dose is controlled by conc. determination after 24 hours (lowest value). | ||||
| 3Supplementary treatment with Vancomycin 15 mg/kg x 3 should be considered in the known carrier of MRSA (not in urinary tract focus) and in suspected care-related KNS infection. Concentration determination before the 4th dose (lowest value). On the basis of the resistance pattern, in some cases you can choose other antibiotics. | ||||
| Patient with renal failure/dialysis: The first treatment week should be done with beta-lactam antibiotics as in normal renal function. For continued dosing during dialysis, see national guidelines information at:Click here! | ||||
Antibiotic Therapy according to Diagnosis and Alternative Therapy when Penicillin Allergy
| Diagnosis | Therapy | Alternative Therapy for PcV allergy |
|---|---|---|
| Pneumonia | Inj. Phenoxymethylpenicilline (Penicilline V) 1 g x 3 i.v. (also with COPD) or T. Penicilline V 1 g x 3 or T. Amoxicillin 500 mg x 3 (patients with COPD) | Inf. Erythromycin (Abboticin) 1 g x 3 i.v. or T. Eryhtromycin 500 mg x 2 or. T. Doxycycline 100 mg x 1 (at COPD; double dose the first day) |
| Pyelonephritis/Febrile Urinary Tract Infection | Inj. Tobramycin (Nebcin*) 4,5 mg/kg x 1 i.v. alt. Inj. Cefotaxime 1 g x 3 i.v. alt. T. Ciprofloxacin 500 mg x 2 | Inj. Tobramycin (Nebcin*) 4,5 mg/kg x 1 i.v. |
| Acute Cystitis | T. Nitrofurantoin (Macrobid) 50 mg x 3 alt. T. Pivmecillinam 200 mg x 3 | |
| Erysipelas (Streptococcus) | Inj. Phenoxymethylpenicilline (Penicilline V) 1-3 g x 3 i.v. alt. T. Penicilline V 1 g x 3 | Inf. Clindamycin 300 mg x 3 i.v. alt. C. Clindamycin 300 mg x 2-3 |
| Skin and soft tissue infection (S. aureus) | Inf. Cloxacillin 2 g x 3 i.v. alt. T. Flucloxacillin 1 g x 3 | Inf. Clindamycin 300 mg x 3 i.v. alt. C. Clindamycin 300 mg x 2-3 |
| Abdominal infection | Inj. Piperacillin/Tazobactam 4 g x 3 i.v. alt. Inj. Cefotaxime 1 g x 3 i.v. + Inf. Metronidazole 1 g x 1 i.v. alt. Inj. Meropenem (Merrem) 0,5 g x 3 i.v. (in case of severe, complicated infection) | Inf. Ciprofloxacin 400 mg x 2 i.v. + Inf. Clindamycin 600 mg x 3 i.v. |
| Severe bacterial infection of unknown origen | Inj. Phenoxymethylpenicilline (Penicilline V) 1 g x 3 i.v. + Inj. Tobramycin (Nebcin*) 4,5 mg/kg x 1 i.v. alt. Inj. Cefotaxime 1 g x 3 i.v. | Inj. Tobramycin (Nebcin*) 4,5 mg/kg x 1 i.v. + Inf. Clindamycin 600 mg x 3 i.v. |
*For severe sepsis, add Nebcina during the first day at a dose of 5-7 mg/kg×1 if Creatinine clearance >80; 4.5-2.2 mg/kg×1 if Creatinine clearance 80-41; 2.2-1 mg/kg×1 if Creatinine clearance 40-20; weight ~ lean body mass. Serum concentration of tobramycin, administered once daily, is measured 8 hours after the dose and should be 1.5-4.0 mg/L at that time.
Duration of antibiotic therapy for common infections
| Infection group | Infection | Population | Recommended duration | Comments |
|---|---|---|---|---|
| Urinary tract | Uncomplicated cystitis | Women/adolescents | Nitrofurantoin – 5 d; TMP-SMX – 3 d; Fosfomycin – 1 d | Young non-pregnant female adolescents or adults with normal urinary tracts and normal renal function |
| Urinary tract | Complicated cystitis | Men | 7 d | Afebrile; urine analysis abnormal and consistent with UTI |
| Urinary tract | Febrile UTI | Children | 7–10 d | Assumes upper tract involvement if febrile |
| Urinary tract | Pyelonephritis and urosepsis | Adults | Initial IV aminoglycoside or ceftriaxone; Quinolones or β-lactams – 7 d | Minimum 7 d, consider longer for slow responders or underlying urinary tract pathology. Excludes patients with stents/drains. |
| Respiratory tract | Streptococcal pharyngitis | Children and adults | 10 d (penicillin V or amoxicillin) | Mainly pediatric studies; some suggest 5 d QID penicillin for eradication only |
| Respiratory tract | Acute otitis media | Children and adults | 6 mo–2 y: 10 d; >2 y: 5 d | Diagnostic criteria incl. fever ≥39°C, bulging tympanic membrane |
| Respiratory tract | Acute sinusitis (uncomplicated) | Children and adults | 5–7 d | Excludes complicated sinusitis (eg, epidural, subdural, orbital); re-evaluate if not improving |
| Respiratory tract | Community-acquired pneumonia (CAP) | Children and adults | 5–7 d | Improved + normal vitals ≥2 d for 5 d course. Same for uncomplicated S. pneumoniae bacteremia. |
| Respiratory tract | Hospital/ventilator-acquired pneumonia (HAP/VAP) | Children and adults | ≤7 d | Consider longer if severely immunosuppressed, abscesses, S. aureus, Pseudomonas |
| Respiratory tract | Acute bacterial COPD exacerbation | Children and adults | 5–7 d | Only for patients meeting criteria for antibiotic treatment |
| Intra-abdominal | Uncomplicated appendicitis | Children and adults | Pre-operative antibiotics only | Gangrenous/perforated without abscess: additional 24–48 h post-op |
| Intra-abdominal | Traumatic bowel perforation | Children and adults | ≤24 h post-op | Operated on within 12 h of trauma |
| Intra-abdominal | Gastroduodenal perforation | Children and adults | ≤24 h post-op | Operated on within 24 h of perforation |
| Intra-abdominal | Intra-abdominal infection/abscess | Children and adults | <7 d after source control | Source control with drainage required. No additional days required if adequate drainage. |
| Skin/Soft tissue | Cellulitis (uncomplicated, non-/purulent) | Children and adults | 5–7 d (unless hospitalized with extensive or severe disease) | Usually due to S. pyogenes if non-purulent, S. aureus if purulent. Incision and drainage with culture recommended for abscesses. |
| Osteoarticular | Acute osteoarticular infections | Children | 3–4 wk | Switch to oral therapy once limb use possible and CRP decreasing. Longer for MRSA or complicated infections. |
| Osteoarticular | Acute vertebral osteomyelitis | Adults | 6 wk | Not associated with implantable device. Typically S. aureus; longer for Salmonella or Brucella. |
| Osteoarticular | Acute native joint osteoarticular infections | Adults | Small joints: 2 wk post-drainage; Large joints: 4 wk post-drainage | Duration recommendation depends on organism and susceptibility profile. |
| Bacteremia | Gram-negative bacteremia (e.g., E. coli, urinary source) | Children and adults | 7 d | Assumes source controlled (eg, line removal, abscess drainage) and not associated with a syndrome requiring longer therapy. Meningitis excluded in infants. |
| Bacteremia | S. aureus bacteremia (uncomplicated) | Children and adults | 14 d IV if uncomplicated or after line removal | Must ensure absence of endocarditis with echocardiogram or other foci. ID consult recommended. Oral step-down possible in children with musculoskeletal infection. |
| Bacteremia | S. aureus bacteremia (complicated) | Children and adults | 4–6 wk IV | Endocarditis, metastatic foci, or persistent bacteremia >72 h despite therapy. ID consult recommended. |
IV = Intravenous; S. pyogenes = Streptococcus pyogenes; CRP = C-reactive protein; MRSA = Methicillin-resistant Staphylococcus aureus; E. coli = Escherichia coli
Classification of bacteria



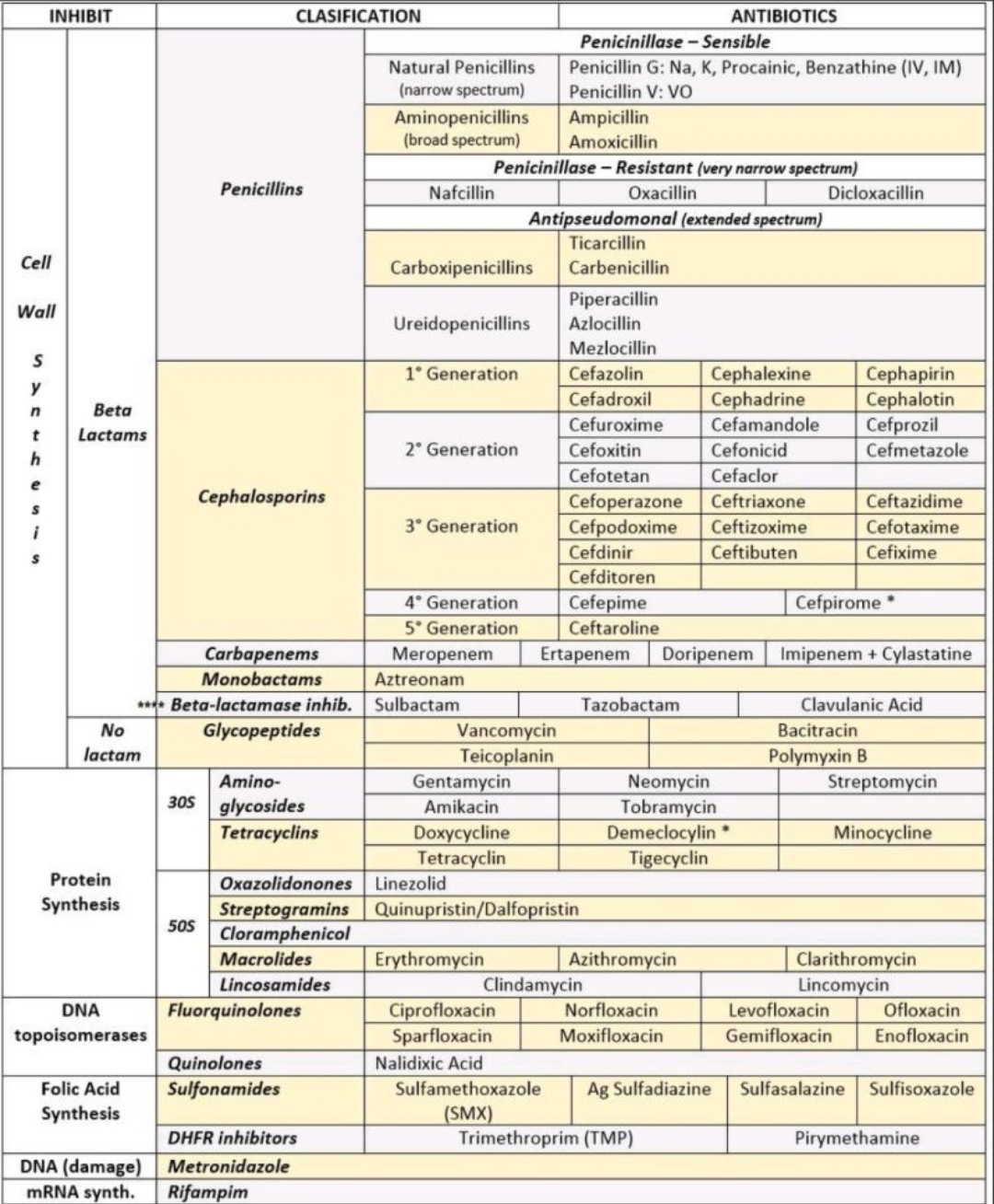
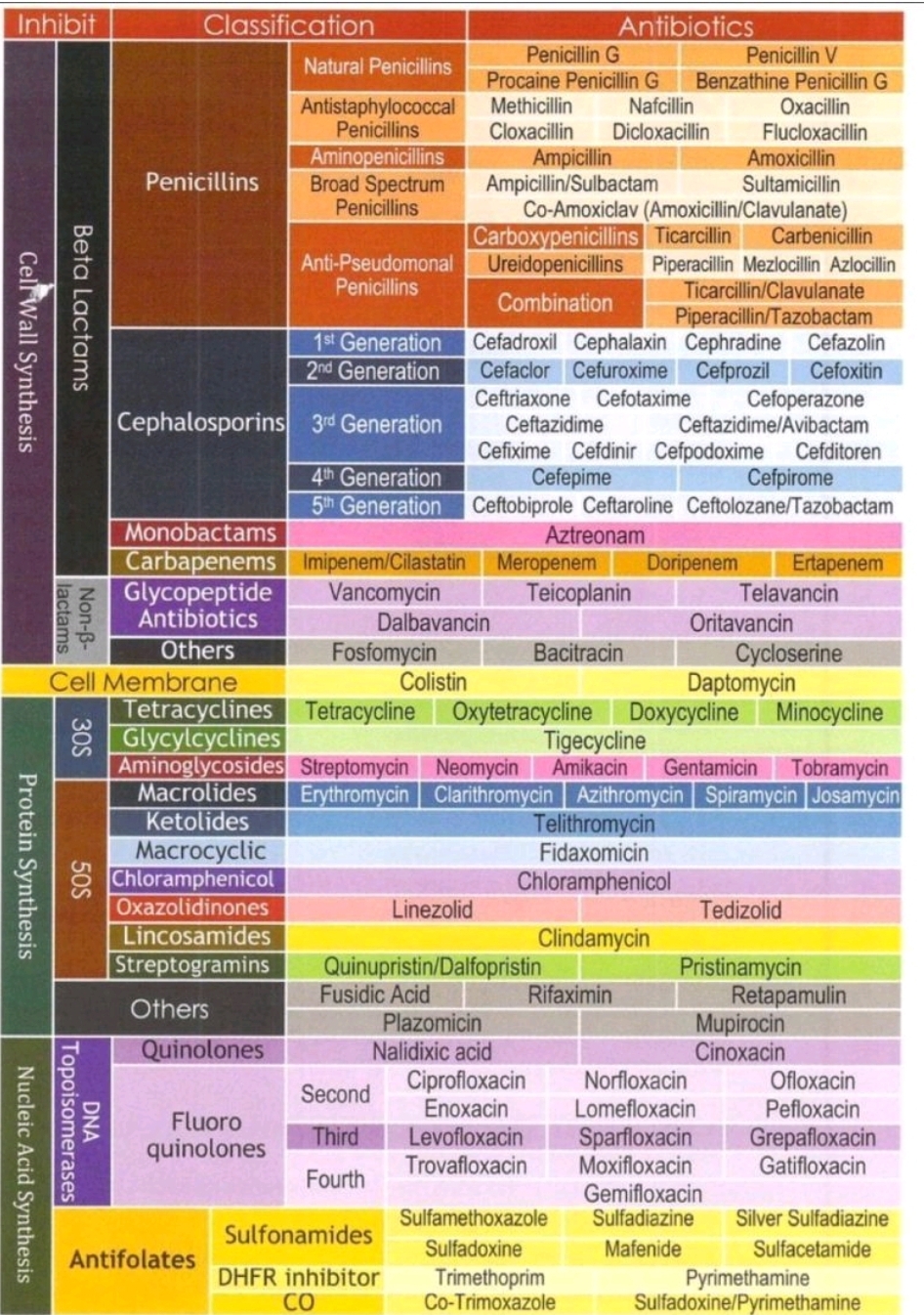
Classification of antibiotics
Sepsis and Septic Shock
Background
Sepsis means that an infection affects the entire body, causing vital organs such as the heart, lungs, brain, and kidneys to malfunction. Even a mild infection can develop into a serious or life-threatening condition. Those affected usually feel very ill and struggle to manage independently. Symptoms often appear suddenly in sepsis, sometimes within a few hours.
Common Symptoms of Sepsis
- Chills
- Fever
- Difficulty breathing, dyspnea, tachypnea
- Confusion
- Diarrhea or vomiting
- Severe abdominal pain, or pain in the back, muscles, or joints
- Muscle weakness (especially in older individuals)
Not all symptoms may be present, but the more symptoms, the higher the likelihood of sepsis. Fever is common, but not everyone will have it.
Sepsis risk stratification
| Parameter | Green light (low risk) | Yellow light (moderate risk) | Red light (high risk) |
|---|---|---|---|
| Behaviour / Level of consciousness | Normal / Alert | History of altered behaviour | Objectively altered behaviour / Not alert |
| Respiratory rate | 12–20 /min | 21–24 /min | ≥25 /min |
| Oxygen saturation on room air | ≥96% | 92–95% | <92% (<88% in COPD) |
| Blood pressure (systolic) | >100 mmHg | 91–100 mmHg | ≤90 mmHg or >40 mmHg below baseline |
| Heart rate | ≤90 /min | 91–130 /min or new-onset arrhythmia | >130 /min |
| Temperature | ≥36°C | <36°C | |
| Urine output | No urine output in the last 12–17 hours | No urine output for ≥18 hours | |
| Skin | Redness; Swelling or discharge from surgical wound; Wound dehiscence | Cyanosis; Mottled or pale skin; Petechial rash | |
| Comorbidity and risk factors | Severe comorbidity; Risk factor | ||
| Social situation | Lack of safety net |
Definition of Sepsis
Sepsis is defined as an infection that triggers a systemic response in the form of:
- Fever/hypothermia >38°C or < 36°C
- Tachycardia > 90 beats per minute
- Increased respiratory rate >20 breaths per minute
- Leukocytes >12 x109/L or <4 x109/L
Early identification and proper treatment of patients with severe sepsis (blood poisoning) reduces mortality. Severe sepsis can affect anyone, but infants and the elderly are at increased risk, as are people with chronic diseases or weakened immune systems. Reliable prevalence data is lacking in Sweden, but it is estimated that 100–300 people per 100,000 inhabitants are affected each year. Mortality in previous studies was reported as very high, with 20% for severe sepsis and 45% for septic shock. Recent studies indicate a mortality rate of around 15-20%. Severe sepsis is one of the most lethal conditions in emergency departments. According to international and national recommendations, patients with severe sepsis should receive proper antibiotic treatment within one hour of arriving at the hospital. Research has shown that early treatment with antibiotics, intravenous fluids, oxygen, and supportive therapy is crucial in severe sepsis. Inadequate initial antibiotic therapy in severe sepsis with a positive blood culture doubles mortality. Delayed appropriate antibiotic treatment in septic shock increases mortality by nearly 8 percentage points per hour during the first 6 hours. The more organ systems fail and the higher the initial lactate level, the higher the mortality rate. This care program describes a sepsis chain for the acute care of patients with or suspected of having severe sepsis and septic shock. The goal is early identification of patients with infections at risk of developing severe sepsis. As part of the sepsis chain, support for management in prehospital, emergency, and correct care placement has been developed. The care chain is supported by cooperation between different parts of healthcare, with a focus on early identification and treatment without delay.
Sequential Organ Failure Assessment SOFA Score
| Organ System | |||||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |
| Respiration | |||||
| paO2/FiO2, kPa | ≥ 53,3 | < 53,3 | < 40 | < 26,7 a | < 13,3 a |
| Coagulation | |||||
| Platelets, × 109/l | ≥150 | <150 | <100 | <50 | <20 |
| Liver | |||||
| Bilirubin, μmol/l | <20 | 20–32 | 33–101 | 102–204 | >204 |
| Circulation | |||||
| Blood Pressure/Catecholamines | Mean arterial pressure ≥70 mm Hg | Mean arterial pressure <70 mm Hg | Dopamine <5 b or dobutamine (regardless of dose) | Dopamine 5,1–15 b or epinephrine ≤0,1 b or norepinephrine ≤0,1 | Dopamine >15 b or epinephrine>0,1 b or noradrenalin >0,1 b |
| CNS | |||||
| Glasgow Coma Scale or | 15 | 13–14 | 10–12 | 6–9 | <6 |
| Reaction Level Scale | 1 | 2 | 3 | 4–5 | 6–8 |
| Renal Function | |||||
| Creatinine, μmol/l and/or diuresis, ml/day | <110 | 110–170 | 171–299 | 300–440 <500 | >440 <200 |
| The original publication for SOFA also requires breathing support for 3 or 4 points [17]. The Swedish Intensive Care Register has chosen to abstain from this requirement, which we propose should apply as general Swedish practice. | |||||
| FiO2 = fraction inspired oxygen; paO2 = partial pressure oxygen in arterial blood. | |||||
| bUnits: μg/kg/min. Catecholamines should have been given for at least 1 hour. | |||||
New definitions diagnostic criteria and codes for sepsis and septic shock according to Sepsis
| Sepsis | Septic Chock | |
|---|---|---|
| Definition | Life-threatening organ dysfunction caused by systemic response to infection | A subset of sepsis where underlying circulatory and cellular / metabolic disorders are sufficiently pronounced to significantly increase mortality |
| Diagnostic Criteria | Acute change infection corresponding to at least 2 SOFA points 1 | Remaining hypotension requiring vasopressor to maintain mean arterial pressure ≥65 mm Hg with lactate> 2 mmol / l despite adequate fluid supply |
| Coding (ICD-10 SE) | R65.1 Sepsis, Sepsis-3 organ failure (increase of at least 2 SOFA scores) Systemic Inflammatory Response Syndrome [SIRS] of Infectious Source with Organ Weight 2 | R57.2 Septic chock |
| 1 If the 2-point increase is achieved by increment of 1 point in two organ systems, these changes should have taken place with sufficient simultaneousity: within 36 hours. SOFA = Sequential organ failure assessment. | ||
| 2 Unfortunately, the old text so far will remain, as it is set by the WHO and is currently unchanged. | ||
When two or more of the above factors are present, the patient meets the criteria for sepsis. However, what we commonly refer to as “sepsis” is actually severe sepsis and septic shock, meaning the infection has caused hypotension, hypoperfusion, and/or organ dysfunction.
The Swedish Infectious Diseases Association has developed guidelines for the assessment of severe sepsis and septic shock as described below. The changes must be caused by the systemic reaction and not be a direct effect of local infection. The changes must be new and not caused by another underlying disease. For the definition of severe sepsis to be met, the patient must have sepsis as defined above, and one or more of the following criteria must be present:

Hypotension
- Systolic blood pressure <90 mm Hg
Organ Dysfunction
- Altered mental status; new-onset confusion, restlessness, aggression, or somnolence
- Renal impairment; creatinine increase >45 μmol/L or oliguria, urine output < 0.5 ml/kg for at least 2 hours despite adequate fluid administration lung impairment:
- pO2 <7.0 kPa on room air (SO2 approximately <86%), pO2 <5.6 kPa on room air (SO2 approximately <78%) if the lungs are the focus of infection
- Coagulopathy; petechiae, ecchymoses, INR >1.5, a-APT time >60 s, or PLT < 100
- Liver dysfunction; s-bilirubin > 45 μmol/L.*
Hypoperfusion
- Lactate >1 mmol above the upper reference limit, or BE ≤-5 mmol/L
- Decreased capillary refill, cold clammy skin, mottling.
*Intestinal impairment (absence of bowel sounds) is considered organ dysfunction in international guidelines, but not in the guidelines of the Swedish Infectious Diseases Association.
The often rapid and unpredictable progression of severe sepsis highlights the importance of clear routines for monitoring vital signs and set thresholds for physician contact and ICU care. It is especially during the first 24 hours after sepsis onset that patients are at risk of deterioration, which justifies enhanced monitoring and readiness to act during this period to prevent the development of:
- Progressing severe sepsis: Worsening of vital signs or rising lactate during the observation period.
- Septic shock: Sepsis with hypotension despite adequate fluid therapy.
Epidemiology
Severe sepsis can affect anyone, but infants and the elderly are at higher risk, as well as people with chronic illnesses or weakened immune systems. Accurate prevalence data is lacking in Sweden, but it is estimated that 100-300 people per 100,000 inhabitants are affected each year.
Preventive Treatment
Appropriate treatment of infections requiring antibiotics without unnecessary delay is important to prevent progression to severe sepsis. The work with STRAMA guidelines is a good tool for outpatient doctors to prescribe antibiotics based on proper indications. Overuse of antibiotics risks creating conditions for the development of antibiotic resistance, which can negatively affect outcomes in severe sepsis. For more information on STRAMA’s guidelines for outpatient care; link
General vaccination programs are crucial in preventing certain severe infectious diseases. Annual influenza vaccination for at-risk groups is particularly important to prevent secondary cases of sepsis, as well as pneumococcal vaccination according to given recommendations. Immunocompromised patients are particularly vulnerable, and it is therefore important that these patients, in case of infection complications, see a doctor with the right expertise to assess the sometimes subtle symptoms that may precede or indicate a serious infection. Furthermore, it is essential to inform patients undergoing immunosuppressive treatment on how to act at the first signs of infection. In some cases, special vaccination may be indicated for immunosuppression.
Symptoms, Clinical Findings, and Early Identification
Severe sepsis is a serious infection characterized by organ damage. Most patients with community-acquired severe sepsis and septic shock are classified as red or orange according to the emergency department’s triage system (RETTS) upon arrival at the emergency department. However, the initial presentation can sometimes be difficult to interpret, and a range of symptoms and clinical findings may occur, which can vary depending on the site of infection, infecting agent, and the patient’s age and comorbidity.
Patients with severe sepsis or septic shock often have a fever or a history of fever and one of the following; elevated heart rate >90/min, elevated respiratory rate >20/min, falling blood pressure, low oxygen saturation <90%, restlessness and confusion, gastrointestinal symptoms such as abdominal pain, diarrhea, or vomiting. With typical symptoms and acute onset with chills, high fever, and general malaise, it is easy to suspect severe sepsis, but many patients, especially the elderly, often present a more atypical picture with, for example, confusion as the only symptom of severe sepsis. It is important to always keep sepsis in mind when examining a critically ill patient with an unclear diagnosis.

Consider the following warning signs of severe infection:
V-BAS; Alertness/Blood Pressure/Respiratory Rate/Saturation or the 90/30/90 Rule:
- Alertness; reduced/new mental impairment
- Systolic blood pressure <90 mmHg
- Respiratory rate >30 breaths per minute
- Oxygen saturation <90%
Sepsis Recognition — 2025 Practical Guide
Section 1: qSOFA vs SIRS — What to Use (and When)
SIRS (Early Screening — Sensitive Detection)
- Temperature >38°C or <36°C
- Heart rate >90/min
- Respiratory rate >20/min or PaCO₂ <32 mmHg
- WBC >12,000 / <4,000 or bands >10%
≥2 + suspected infection = THINK SEPSIS
qSOFA (Bedside Risk Tool — Severity & Prognosis)
- Respiratory rate ≥22/min
- Altered mentation (GCS <15)
- Systolic BP ≤100 mmHg
≥2 = HIGH MORTALITY RISK (Not diagnostic)
qSOFA is not a screening tool
Section 2: Lactate — Targets & Interpretation
- Measure within 1 hour
- Recheck every 2–4 hours
⚠ ≥2 mmol/L → Tissue hypoperfusion
⚠ ≥4 mmol/L → High risk of septic shock (even if BP normal)
🎯 Goal: Downward trend / lactate clearance ≥10%
⚠ Pitfall: Normal BP ≠ normal perfusion (cryptic shock). Trust lactate.
Section 3: Fluids — How Much, How Fast (Updated View)
- Start 20–30 mL/kg balanced crystalloids
→ Give in boluses with frequent reassessment
Dynamic assessment tools:
- Capillary refill time
- Passive leg raise
- IVC variation (if skilled)
🚫 Avoid blind large-volume resuscitation
🛑 Stop if pulmonary edema, worsening venous congestion, or worsening oxygenation
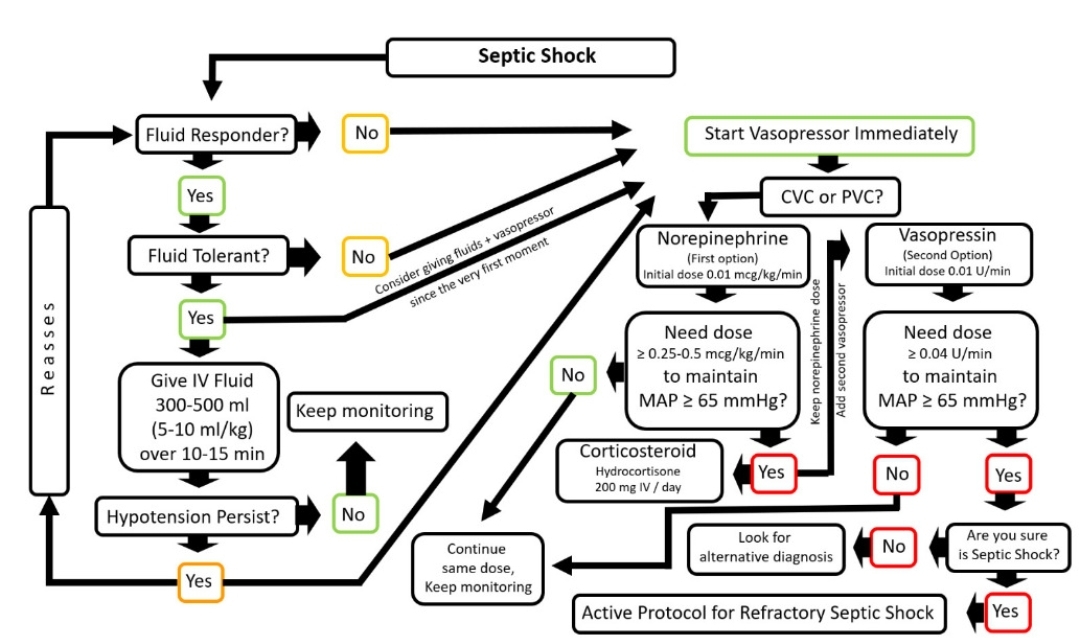
Section 4: Vasopressor Sequencing (Early, Not Late)
- 1st line: Norepinephrine
If MAP <65 mmHg persists:
- Add Vasopressin (fixed dose)
- Then Epinephrine if required
Refractory shock:
- Consider Hydrocortisone 200 mg/day
🎯 Target MAP ≥65 mmHg
(Individualize in chronic hypertensives)
Section 5: Antibiotics — Timing Matters More Than Choice
- Start within 1 hour
- Broad-spectrum initially
- De-escalate at 48–72 hours
- Send cultures before antibiotics if no delay
⚠ Missing source control = treatment failure
Section 6: Common Pitfalls (High-Yield)
❌ Delayed recognition of shock
❌ Over-resuscitation with fluids
❌ Ignoring lactate trends
❌ Delayed vasopressors
❌ Missing occult sources (lines, abdomen, urine, lung)
❌ Attributing delirium to “ICU psychosis”
Key message:
💡 Sepsis is a perfusion problem first, a blood-pressure problem later.
Sepsis Alarm
For early identification, sepsis alarms should be used, which involve a modified version of RETTS focusing on patients at risk of serious infection. RETTS (Rapid Emergency Triage and Treatment System) is the triage system used in many emergency departments across the country. RETTS is based on vital signs (blood pressure, pulse, respiratory rate, alertness, and temperature) with specified thresholds to sort patients into the correct priority group. Red RETTS means that the patient’s oxygen saturation is below 90% despite oxygen treatment, respiratory rate is over 30 or under 8, blood pressure <90 mm Hg, pulse >130, or that the patient is having seizures or is unconscious.
In addition to vital signs, an ESS (Emergency Signs and Symptoms) should be added. For severe sepsis, ESS 47 (infection, fever, local infection) is applied. ESS 51 should also be applied (known adrenal insufficiency, immunodeficiency, or immunosuppression), which finally determines the patient’s priority.
A sepsis alarm is triggered in patients with red RETTS who have a fever or a history of fever. In these cases, the patient is triaged according to a special algorithm, and an infectious disease specialist/emergency physician is called to the emergency room immediately upon the patient’s arrival.
By focusing early on patients who have or are at risk of severe sepsis, it is ensured that the patient receives appropriate antibiotics within 60 minutes after blood cultures (2+2) are taken, and that correct supportive treatment is initiated and continues with intravenous fluids and oxygen.
SOME POINTS TO KEEP IN MIND TO AVOID MISSING PATIENTS WITH SEVERE SEPSIS
- Fever (>38.0°C) is not always present, and ear thermometers are unreliable. Hypothermia (<36.0°C) can be a serious sign in severe sepsis.
- “Found on the floor” may be secondary to sepsis
- Sepsis-induced confusion can be mistaken for a stroke.
- Remember that gastrointestinal symptoms and flu-like conditions may be due to severe sepsis.
- CRP may be normal or only moderately elevated initially.
- Check the skin – petechiae? Infected wounds?
- Consider reduced immune response in certain groups such as patients with rheumatic systemic diseases, IBD, malignant tumors, transplanted patients, splenectomized patients, and patients on current or recent treatment with immunomodulating drugs such as Prednisolone 15 mg or more, Methotrexate®, Remicade® (infliximab), Enbrel® (etanercept), cytostatics, and others.
Primary Measures
- Monitoring – follow blood pressure, pulse, oxygen saturation, alertness!
- Establish peripheral intravenous access.
- Oxygen 2–5 liters via nasal cannula, >5 liters via mask, target saturation >93%. Use caution with COPD! Inform the emergency department if the patient has COPD.
- Infusion of Ringer’s acetate, if BP <90 mm Hg, administer a bolus dose of 500–1,000 ml over 30 minutes, repeat until treatment goal is reached, i.e., BP >90 mm Hg. In total, at least 30 ml/kg IV should be given within 3 hours in severe sepsis with hypotension.
- Paracetamol should only be given if the patient is clinically affected by the fever or in cases of ongoing cerebral ischemia/seizure/cardiac ischemia.
PREHOSPITAL IDENTIFICATION AND MANAGEMENT
- Suspected infection is generally identified using RETTS
- Vital signs should also include ESS 47, which determines the patient’s priority. In some cases, ESS 51 (known adrenal insufficiency, immunodeficiency, or immunosuppression) should be used.
- In addition to this analysis, note the following criteria as signs of suspected severe infection:
Fever (temp >38.0°C) or low temp (<36.0°C)/history of fever and any of the following symptoms/signs:
- Petechiae/rash
- Signs of infected skin/soft tissue/joints
- New onset of severe pain
- Cerebral impairment/severe headache
- Urinary symptoms (especially with an indwelling catheter)
- Central venous catheter or other invasive port with signs of infection
Epidemiology? Always ask about recent travel abroad!
Remember that fever may be absent in immunocompromised patients and in patients who have taken paracetamol and NSAIDs, and that diarrhea/abdominal pain/vomiting are common symptoms of severe sepsis.
- Oxygen, adjusted according to saturation, 2–5 liters via nasal cannula, >5 liters via mask, target saturation >93%. Use caution with COPD! Inform the emergency department if the patient has COPD.
- Establish peripheral intravenous access.
- Consider intraosseous access if there is difficulty with IV access in critically ill patients who urgently need access for fluid/medication administration.
- Infusion of Ringer’s acetate, if BP <90 mm Hg, administer a bolus dose of 500–1,000 ml over 30 minutes, repeat until treatment goal is reached, i.e., BP >90 mm Hg. In total, at least 30 ml/kg IV should be given within 3 hours in severe sepsis with hypotension.
- Avoid the general prescription of paracetamol for fever. Antipyretics should only be given if the patient is clinically affected by the fever or in cases of ongoing cerebral ischemia/seizure/cardiac ischemia.
Intrahospital Diagnosis and Treatment
- Initial management according to A – B – C – D – E
- Peripheral intravenous access x 2
- Consider central venous catheter (CVC) or intraosseous access if difficulty with IV access in critically ill patients urgently needing access for fluid/medication administration.
- Blood cultures 2+2
- Arterial or venous blood gas for lactate analysis.
- Blood tests; CRP, white blood cell count, platelets, prothrombin time (PT), activated partial thromboplastin time (APTT), liver function tests, urine dipstick, blood glucose.
- Urine culture (if needed, catheterization) and other relevant cultures as per doctor’s orders.
- Is there a suspected bacterial infection? Assess the infection focus. After appropriate cultures, consider antibiotics as per point 15.
- If meningitis is suspected, perform lumbar puncture (LP); see national guidelines at www.infektion.net
- ECG
- Consider chest X-ray bedside.
- Vital signs every 5 minutes initially until the patient is stabilized.
- Epidemiology? Always ask about recent travel abroad!
- Remember that fever may be absent in immunocompromised patients and in patients who have taken paracetamol and NSAIDs, and that diarrhea/abdominal pain/vomiting are common symptoms of severe sepsis.
Treatment
- The infectious disease specialist/emergency doctor* joins the emergency room during a sepsis alarm. If there is no infectious disease specialist available at the hospital, contact the specialist by phone for advice on investigation and antibiotic selection, especially for immunocompromised patients or those suspected of carrying resistant bacteria.
- Oxygen, adjusted according to saturation, 1–5 liters via nasal cannula, >5 liters via mask, treatment goal >93%. Use caution with COPD!
- Infusion of Ringer’s acetate, if BP <90 mm Hg, administer a bolus dose of 500–1,000 ml over 30 minutes, repeat until treatment goal BP >90 mm Hg is reached. In total, at least 30 ml/kg IV should be given within 3 hours in severe sepsis with hypotension or lactate >4.
- Choice of antibiotics is based on the severity of the infection and the suspected focus.
If antibiotics are prescribed, they should be administered without delay in the emergency department!
- Consider invasive management of the infection focus (so-called source control) in cases such as septic arthritis, abscess, obstructive pyelonephritis, empyema, bowel perforation, gynecological infection, or necrotizing fasciitis.
- If the patient is on or has recently finished treatment with corticosteroids, administer Solu-Cortef 100 mg IV.
- Insert a urinary catheter and attach a bag for monitoring urine output, target 0.5 ml/kg/hour.
- Administer Albumin 20% 100 ml if hypotension persists after 2–3 liters of Ringer’s acetate. Do not use starch solutions (e.g., Voluven). If Albumin is not available, continue with Ringer’s acetate.
- Avoid the general prescription of paracetamol for fever. Antipyretics should only be given if the patient is clinically affected by the fever or in cases of ongoing cerebral ischemia/seizure/cardiac ischemia.
*Which doctor is called depends on the respective hospital; if an infectious disease specialist is available, they should be called. Otherwise, the medical or emergency doctor should be contacted according to local guidelines.
Care Level – Admission
- Decision on the level of care: ICU/intermediate care or general ward.
- Transfer to the infectious disease ward, emergency care ward, or another ward with sufficient monitoring resources without delay. While waiting for transfer, check vital parameters every 15 minutes.
- Evaluate if treatment limitations are necessary.
The Emergency Room – Continued Deterioration of Vital Functions After Initial Measures
Establish contact with the Medical Emergency Team (MET) or ICU consultant (infectious disease consultant) to assess the need for ICU care.
- If BP <90 despite IV fluids or saturation <90 despite oxygen therapy
- If lactate >4 or increasing
- If respiratory rate >30 despite treatment
- In cases of severe organ dysfunction such as reduced consciousness
Diagnostics
- Peripheral IV access x2
- Blood culture 2+2
- Arterial or venous blood gas for lactate analysis, if >3.5 the patient should be upgraded to red RETTS and a sepsis alarm should be triggered, see above.
- Blood tests: CRP, leukocytes, platelets, prothrombin time (PT), activated partial thromboplastin time (APTT), liver function tests, urine dipstick, blood glucose
- Urine culture (with catheter if needed) and other relevant cultures as per the doctor’s orders.
- Is there a suspected bacterial infection? Evaluate the infection focus. After appropriate cultures, decide on antibiotics as per point 15.
- If meningitis is suspected, perform a lumbar puncture (LP), see national guidelines at www.infektion.net
- Vital parameters and monitoring at 15-minute intervals.
- Epidemiology? Always ask about recent travel abroad!
- Remember that fever may be absent in immunocompromised patients and in patients who have taken paracetamol and NSAIDs, and that diarrhea/abdominal pain/vomiting are common symptoms of severe sepsis.
Treatment
- During the day, primarily handled by the infectious disease day consultant*, during on-call hours consult the infectious disease consultant by phone, who will assess the patient in the emergency room if necessary, especially for immunocompromised patients and those known to carry resistant bacteria.
- Oxygen, adjusted according to saturation, 1–5 liters via nasal cannula, >5 liters via mask, target saturation >93%. Use caution with COPD!
- Infusion of Ringer’s acetate 1,000 ml, a total of at least 30 ml/kg IV should be given within 3 hours in severe sepsis with hypotension or lactate >4.
- Antibiotic choice is based on the severity of the infection and the suspected focus.
If antibiotics are prescribed, they should be administered without delay in the emergency room!
- Consider invasive management of the infection focus (so-called source control) in cases such as septic arthritis, abscess, obstructive pyelonephritis, empyema, bowel perforation, gynecological infection, or necrotizing fasciitis.
- If the patient is on or has recently finished treatment with corticosteroids, administer Solu-Cortef 100 mg IV.
- Antipyretics should only be given if the patient is clinically affected by the fever or in cases of ongoing cerebral ischemia/seizure/cardiac ischemia. Avoid general prescriptions for fever.
*Which consultant is called depends on the respective hospital. Where available, an infectious disease consultant should be contacted. Otherwise, consult the medical or emergency consultant according to local guidelines.
Antibiotic Treatment in the Intensive Care Unit
Community Acquired Infection with Severe Sepsis or Septic Shock
| Infection | Suggestion of Antibiotics |
|---|---|
| Sepsis of unknown origen | A) Piperacilline/Tazobactam 4 g x 4 + Tobramycin (Nebcin®) 5-7 mg/kg x 1 B) Meropenem 1 g x 4 + Tobramycin (Nebcin®) 5-7 mg/kg x 1 |
| Pneumonia | A) Cephotaxime 1 g x 3 + Erythromycin (Abboticin®) 1 g x 3 + Tobramycin (Nebcin®) 5-7 mg/kg x 1 B) Phenoxymethylpenicilline 3 g x 4 + Moxifloxacin (Avelox®) 400 mg x 1 + Tobramycin (Nebcin®) 5-7 mg/kg x 1 |
| Abdominal infection | A) Piperacillin/Tazobactam 4 g x 3 + Tobramycin (Nebcin®) 5-7 mg/kg x 1 B) Meropenem 1 g x 4 + Tobramycin (Nebcin®) 5-7 mg/kg x 1 |
| Fasciitis/myositis | A) Meropenem 1 g x 4 (alt. Phenoxymethylpenicilline 3 g x 4 with verified grp A strpc) + Clindamycin 600 mg x 3 + Tobramycin 5-7 mg/kg x 1 (not with Strpc A) |
| Meningitis | Meropenem 2 g x 3 |
Community Acquired Infection without Severe Sepsis or Septic Shock
| Infection | Choice of Antibiotics |
|---|---|
| Sepsis of unknown origen | Piperacillin/Tazobactam 4 g x 3-4 |
| Pneumonia | A) Cephotaxime 1 g x 3 + Erythromycin (Abboticin®) 1 g x 3 B) Phenoxymethylpenicilline 3 g x 4 + Moxifloxacin (Avelox®) 400 mg x 1 + |
| Abdominal infection | A) Piperacillin/Tazobactam 4 g x 3 B) Cephotaxime 1 g x 3 + Metronidazol 1.5 g x 1 C) Meropenem 0.5 g x 3 |
| Fasciitis/myositis | Meropenem 1 g x 4 (alt. Phenoxymethylpenicilline 3 g x 4 at verif group A strpcocc) + Clindamycin 600 mg x 3 |
| Meningitis | Meropenem 2 g x 3 |
Nosocomial Infection Hospital Acquired (> 48 hours in hospital)
| Infection | Choice of Antibiotics |
|---|---|
| Sepsis of unknown origen | A) Meropenem 0,5-1 g x 3-4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg x 1 B) Piperacillin/Tazobactam 4 g x 3 + ev. Tobramycin (Nebcin®) 5-7 mg/kg x 1 |
| Pneumonia | A) Piperacillin/Tazobactam 4 g x 3-4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg x 1 B) Meropenem 0,5-1 g x 3-4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg x 1 |
| Abdominal infection | A) Piperacillin/Tazobactam 4 g x 3-4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg x 1 B) Meropenem 0,5-1 g x 3-4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Fasciitis/myositis | Meropenem 1 g x 3-4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Meningitis | Meropenem 2 g x 3 + Vancomycin 1 g x 3 (after Neurosurgery) |
Immune Deficiency Patients with Neutropenia
| Infection | Choice of Antibiotics |
|---|---|
| Sepsis of unknown origen | A) Meropenem 0,5-1 g x 4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg B) Piperacillin/Tazobactam 4 g x 4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Pneumonia | A) Meropenem 0,5-1 g x 4 + Erythromycin (Abboticin®) 1 g x 3 + ev. Tobramycin (Nebcin®) 5-7 mg/kg B) Piperacillin/Tazobactam 4 g x 4 + Erythromycin (Abboticin®) 1 g x 3 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Abdominal infection | A) Piperacillin/Tazobactam 4 g x 4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg B) Meropenem 0,5-1 g x 4 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Fasciitis/myositis | Meropenem 1 g x 4 (alt. Phenoxymethylpenicilline 3 g x 4 at verif group A strpk) + Clindamycin 600 mg x 3 |
| Meningitis | Meropenem 2 g x 3 |
Serious Penicillin Cefalosporin Allergy
| Infection | Choice of Antibiotics |
|---|---|
| Sepsis of unknown origen | Clindamycin 600 mg x 3 + Ciprofloxacin 400 mg x 3 + Tobramycin (Nebcin®) 5-7 mg/kg |
| Pneumonia | Clindamycin 600 mg x 3 + Moxifloxacin (Avelox®) 400 mg x 1 (vid VAP Ciprofloxacin 400 mg x 3) + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Abdominal infection | Clindamycin 600 mg x 3 + Ciprofloxacin 400 mg x 3 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Fasciitis/myositis | Clindamycin 600 mg x 3 + Ciprofloxacin 400 mg x 3 + ev. Tobramycin (Nebcin®) 5-7 mg/kg |
| Meningitis | A) Meropenem 2 g x 3 (not at anaphylactic shock of PcV) + Vancomycin 1 g x 3 B) Moxifloxacin (Avelox®) 400 mg x 1 + Vancomycin 1 g x 3 + Trimetoprim Sulfametoxazol 20 ml x 2 |
Note: Always take cultures from relevant locations before starting antibiotic treatment, such as blood, sputum, wound, and urine.
In cases of severe sepsis, add Nebcina during the first 24 hours at a dose of 5-7 mg/kg×1 if creatinine clearance >80; 4.5-2.2 mg/kg×1 if creatinine clearance 80-41; 2.2-1 mg/kg×1 if creatinine clearance 40-20; weight ~ lean body mass. Tobramycin serum concentration, administered once daily, is measured 8 hours after the dose and should be 1.5-4.0 mg/L at that time.
The dosing instructions assume an adult patient with normal kidney function. Creatinine clearance (ml/min) = F x (140-age) x weight/S-creatinine; F≈1.2 for men; F≈1.0 for women.
In cases of increased risk for ESBL-producing gut bacteria (foreign travel, foreign hospital care, known colonization): Meropenem 1g x 4 + amikacin (Biklin) 20-25 mg/kg x 1. In cases of fasciitis/myositis, consult the infectious disease specialist for consideration of IV immunoglobulin. For meningitis, always add dexamethasone (Betapred) 8 mg x 4.
Higher doses and more frequent dosing are required for severe sepsis/septic shock due to increased distribution volume and impaired microcirculation. Usually, lower/less frequent dosing is needed later in the course. Add Nebcina 1 dose/day for severe sepsis/septic shock. Normal dose 7 mg/kg. Lower dose (5 mg/kg) in older patients or those with chronic kidney disease. Avoid Nebcina if GFR <20 ml/min. For treatment with Biklin, take trough concentration just before the next dose.
Antibiotic Choice in Severe Sepsis
Severe sepsis and septic shock are very serious conditions that require early, correct treatment. It is important to start with broad-spectrum antibiotic therapy.
Check for previous colonization with resistant bacteria and review the microbiology domain, also evaluate local resistance patterns.
Contact the infectious disease consultant when managing patients with progressing severe sepsis and septic shock, especially when the infection is suspected to be caused by resistant bacteria or in immunocompromised patients . The following antibiotic dosing applies to initial management; continued dosing and antibiotic treatment in cases of persistent severe sepsis or septic shock should be discussed with the infectious disease consultant.
The following antibiotic suggestions apply only in cases of severe sepsis and septic shock. For correct treatment, see previous definitions on p. 6. Aim for targeted treatment if the infection focus is suspected. Generally, higher initial antibiotic doses and more frequent dosing (an extra dose after 4 hours, the next dose 4 hours later, when treating with beta-lactam antibiotics such as Benzylpenicillin, Cefotaxime, Piperacillin/Tazobactam, and Meropenem/Imipenem) are recommended in severe sepsis/septic shock as the distribution volume in these conditions is increased, leading to low tissue concentrations with standard dosing. When stabilized, normal dosing applies. For more detailed information, see the national care program at www.infektion.net.
ANTIBIOTIC CHOICE FOR PATIENTS WITH SEVERE SEPSIS OR SEPTIC SHOCK**
Antibiotic Selection in Severe Sepsis
| Source of Infection | Antibiotic Choice |
|---|---|
| Suspected pneumonia | Cefotaxime 2 g + Tavanic 0,5 g |
| Suspected Urosepsis** | Cefotaxime 2 g + Amino Glycoside* 4,5-7 mg/kg |
| Suspected Abdominal Foci** | Piperacilline/Tazobactam 4 g/Meropenem 1 g/Imipenem 1 g + ev. Single Dose of Amino Glycoside* 4,5–7 mg/kg |
| Suspected skin/Soft tissue infection | Suspected Streptococcal genesis: Phenoxymethylpenicilline-pcV 3 g + Clindamycine 600 mg Suspected Staf. Aureus genesis Cloxacilline 2 g + Clindamycine 600 mg Suspected Fasciitis/Myositis Meropenem/Imipenem 1 g + Clindamycine 600 mg + ev. Amino Glycoside* 4,5–7 mg/kg |
| Suspected meningitis | Cefotaxime 3 g + Ampicilline 3 g + Betametason |
| Unknown Foci** | Piperacilline/Tazobactam 4 g/Meropenem 1 g/Imipenem 1 g + Amino Glycoside* 4,5–7 mg/kg. In a stable patient with rapid transient organ failure, treatment with Cefotaxime 2 g + Amino Glycoside* 4.5 mg/kg may be considered. |
| Unknown foci and Type 1 hypersensitivity to Penicilline | Clindamycine 600 mg + Ciprofloxacin 400 mg + Hypersensitivity to penicillin: a dose Amino Glycoside* 4,5–7 mg/kg |
* Use the higher dose of aminoglycosides in cases of progressing severe sepsis and septic shock. In milder cases of severe sepsis that respond well to initial fluid therapy, aminoglycosides can be withheld.
** If current or previous colonization with ESBL-producing pathogens is suspected, Meropenem/Imipenem 1g should be administered initially. If risk factors for infection caused by ESBL-producing pathogens, such as a history of travel to regions with a high prevalence of antibiotic resistance or residence in a nursing home with a high prevalence of resistant bacteria, consult an infectious disease specialist.
ANTIBIOTIC CHOICE IN PREGNANT PATIENTS WITH SEVERE SEPSIS OR SEPTIC SHOCK
Penicillins, cephalosporins, carbapenems, and clindamycin are safe to administer. A single dose of aminoglycosides can be considered if the indication is strong. Consult an infectious disease specialist. Avoid quinolones throughout pregnancy, and avoid macrolides during the first trimester (doxycycline can be given in the first trimester but should be avoided in the second and third trimesters), see www.infpreg.se.
ANTIBIOTIC CHOICE IN PATIENTS WITH RENAL FAILURE AND SEVERE SEPSIS OR SEPTIC SHOCK
Renal failure is very common in severe sepsis and septic shock. In principle, the first dose can always be given as a full dose, but subsequent doses must be adjusted according to kidney function.
ANTIBIOTIC CHOICE IN SEVERELY OBESE PATIENTS WITH SEVERE SEPSIS OR SEPTIC SHOCK
There is uncertainty regarding optimal antibiotic doses in severely overweight/obese patients. The Swedish Infectious Disease Association recommends adjusting the dose of certain antibiotics for patients with a BMI >30 kg/m2 (BMI=weight/height2). Consult an infectious disease specialist for advice.
ANTIBIOTIC CHOICE IN PATIENTS WITH SEPSIS WITHOUT ORGAN DYSFUNCTION (FEBRILE BACTERIAL INFECTION)
Antibiotic Selection in Moderate Sepsis without Organ Failure
| Source of Infection | Antibiotic Choice |
|---|---|
| With unknown origen | Phenoxymethylpenicillin 1-3 g + Amino Glycoside 4.5 mg/kg alternatively Cefotaxime 1 g if risk factors for Amino Glycoside related side effects are known as known hearing loss or chronic renal impairment. |
| With suspected focus; for example pneumonia, febrile UVI / pyelonephritis, erysipelas. | Antibiotic treatment in accordance with local guidelines or STRAMA Guidelines for infections in hospitalized patients. |
Other Treatments in Severe Sepsis
- DVT prophylaxis: Low molecular weight heparin and compression stockings should be given to all patients with severe sepsis unless there is a risk of bleeding or other contraindications.
- PPI: If PT >1.5 or platelets <50 or hypotension is present, PPI (proton pump inhibitor) is given as ulcer prophylaxis, Nexium 40 mg x 1 IV. The treatment should be discontinued when the patient is stabilized and able to eat per os.
- Blood glucose control: Aim for glucose levels <10 mmol/L.
Ethical Considerations in Severe Sepsis
The care program is a support for initial management, and it is essential that ethical principles, the prognosis of any underlying chronic diseases, and the prognosis of the acute illness are considered. Each patient should be assessed individually regarding appropriate care interventions and care level. Deviations from treatment should be justified and documented.
In the group of elderly patients with multiple illnesses, it is not uncommon for the patient to, after careful consideration, decline acute hospital care. In such cases, treatment at home with support from a mobile elderly care team can be arranged where possible. If this care is unavailable, the care should be adapted as best as possible given the circumstances.
Follow-up
Proper monitoring while awaiting a hospital bed and evaluation of treatment effectiveness through lactate level checks and vital parameters in accordance with the patient’s RETTS score.
A reasonable treatment goal is for the patient to have a systolic blood pressure >90 mmHg and oxygen saturation >93% (not applicable to COPD patients) within 1 hour of treatment initiation. Within 6 hours, urine output should be adequate >0.5 ml/kg/hour, and any elevated lactate value should have decreased. After 3–6 hours, the responsible physician should assess whether the patient has met the treatment goals. The risk of rapid deterioration is highest during the first 24 hours in the hospital. If vital parameters are deteriorating, NEWS >6, contact the Medical Emergency Team (MET) and the infectious disease consultant by phone.*
Before the patient leaves the emergency department, a NEWS assessment should be performed, and upon arrival at the ward, a NEWS assessment should be repeated. During handover to the ward, clear levels for ongoing fluid treatment, oxygen therapy, target levels for oxygen saturation and blood pressure, as well as when the next antibiotic dose should be given and in what dose, along with intervals for NEWS assessments, should be communicated.
*Which consultant is called depends on the respective hospital. If an infectious disease consultant is available, they should be contacted. Otherwise, contact the medical or emergency consultant according to local guidelines.
- Surviving Sepsis Campaign, via the link http://www.survivingsepsis.org
- Infectious Disease Society’s care program, version 2013 via the link www.infektion.net
- Glickman et al 2010, Acad Emerg Med. 2010 Apr;17(4):383-90. doi: 10.1111/j.1553-2712.2010.00664
- Widgren B et al. The Journal of Emergency Medicine, 2011;40:623-628.
Bacterial Sensitivity to Various Antibiotics


The tables above show bacterial sensitivity to various antibiotics. Published with permission from UAS. The images are clickable for a more detailed view in higher resolution. Different colors indicate classes of antibiotics.
Classification of Bacteria by Cocci/Rods, G +/-, Aerobic/Anaerobic

Antibiotics for Reduced Renal Function
Antibiotics in case of impaired renal function
| Creatinine Clearance (ml/min) | > 80 ml/min | 80-41 ml/min | 40-20 ml/min | < 20 ml/min |
|---|---|---|---|---|
| Ampicillin | 2 g x 3 | 2 g x 3 | 2 g x 2 | 1 g x 2 |
| Phenoxymethylpenicilline | 1 g x 3 | 1 g x 3 | 1 g x 2 | 1 g x 2 |
| Cloxacillin | 2 g x 3 | 2 g x 3 | 1 g x 3 | 1 g x 3 |
| Piperacillin + tazobactam | 4 g x 3 | 4 g x 3 | 4 g x 3 | 4 g x 2 |
| Cefotaxime | 1 g x 3 | 1 g x 3 | 1 g x 2 | 1 g x 2 |
| Ceftazidime at neutropenia | 1 g x 3 1 g x 4 | 1 g x 2 1 g x 3 | 0,5 g x 2 0,5 g x 3 | 0,5 g x 1 0,5 g x 2 |
| Meropenem at neutropenia | 0,5 g x 3 0,5 g x 4 | 0,5 g x 3 0,5 g x 4 | 0,5 g x 2 0,5 g x 3 | 0,25 g x 2 0,5 g x 2 |
| Ciprofloxacin | 400 mg x 2 | 400 mg x 2 | 400 mg x 1 | 400 mg x 1 |
| Tobramycin* | 6-4,5 mg/kg x 1 | 4,5-2,2 mg/kg x 1 | 2,2-1 mg/kg x1 |
Antibiotics independent of renal function
| Generic Substance | Different label names: | |||
|---|---|---|---|---|
| Doxycycline | Doxyferm | Doryx | Doxyhexal | Doxylin |
| Erytromycin | Ery-Max | Eryc | Erythrocin | |
| Fucidin | Fucidin | Fucithalmic | Stafine | |
| Clindamycin | Clindamycin | Cleocin | Dalacin | Clinacin |
| Metronidazole | Flagyl | Metro | ||
| Rifampicin | Rimactan | Rifadin | ||
High bioavailability after oral administration
| Generic Substance | Different label names: | |||
|---|---|---|---|---|
| Doxycycline | Doxyferm | Doryx | Doxyhexal | Doxylin |
| Fluconazol | Fluconazol | |||
| Clindamycin | Clindamycin | |||
| Metronidazol | Flagyl | Metro | ||
| Trimetoprim Sulfametoxazol | Eusaprim | Bactrim | ||
Parenteral Antibiotics for Children
| Medication | Concentration | Dose | Note |
|---|---|---|---|
| Erythromycin | 10-15 mg/kg x 3 | Caution in liver failure and in heart disease (arrhythmias). Dose reduction in renal impairment. | |
| Phenoxymethylpenicilline (Bensyl PCV) | 100 mg/ml | 25-50 mg/kg x 3 (3g x 3) alt. 50-100 mg/kg x 4 (3 g x 4) | |
| Cefotaxime | 100 mg/ml | 30 mg/kg x 3. (1g x 3) alt. 75-100 mg/kg x 3 (3 g x 3) | |
| Ceftazidime | 100 mg/ml | 25 mg/kg x 3 (1 g x 3) alt. 50 mg/kg x 3 (2 g x 3) alt. 35 mg/kg x 3 (2 g x 3) Children< 2 months: 25 mg/kg x 2 | Diluted with sterile water. Given for 3-5 min. |
| Cefuroxime | 100 mg/ml | 20-30 mg/kg x 3 (0,75-1,5 g x 3) | Diluted with sterile water. Given for 3-5 min. |
| Clindamycin | 10 mg / kg x 3 (600 mg x 3) No child <4 weeks age | ||
| Cloxacillin | 50 mg/ml | Diluted with sterile water. Given in CVC 3-5 min. All infusion in pvc: Then dilute once more with NaCl 9mg/ml to 20 mg/ml. 20-30 min. | |
| Meropenem | 50 mg/ml | 40 mg/kg x 3 (2 g x 3) alt. 20 mg/kg x 3-4 (2 g x 3-4) alt. 10-20 mg/kg x 3 (0,5-1 g x 3) | Diluted with sterile water. Given for 3-5 min. |
| Tobramycin | 10 mg/ml | 7.5 mg/kg x 1. Higher dose 8-10-(12) mg/kg x1 can be used in CF and neutropenic fever. | Nebcina 40 mg/ml is diluted with NaCl 9 mg/ml alt. Glucose 50 mg/ml. Infusion for 20-60 min. |
| Vancomycin | 5 mg/ml | 20 mg/kg x 2 (-3) (1 g x 2) ev x 3 | Diluted in two steps. First stock solution with sterile water to 50 mg/ml. Then dilute with sodium chloride 9 mg/ml or glucose 50 mg/ml to 5 mg/ml. Infusion for at least 60 minutes. |
| Piperacillin/Tazobactam | 80 mg/kg x 3-4 alt. 100 mg/kg x 3-4 (4 g x 3-4) | ||
| Ceftriaxone | 100 mg/kg x 1. (2 g x 1) | ||
| Linezolid | 10 mg/kg x 2 (600 mg x 2) | (max 28 days) |
Fungal Infections in Intensive Care
Fungal infections and fungal sepsis are common in intensive care, especially in patients receiving prolonged treatment with broad-spectrum antibiotics, immunocompromised patients, those in poor nutritional status, or those with extensive necrosis or burns. Antifungal agents are often added to the treatment of ICU patients. The presence of deep fungal infection can be confirmed with beta-glucan testing. Beta-glucan is a fungal antigen that can be detected in the blood in cases of invasive fungal infection. Values above 100 pg/mL are considered positive, while values below 100 pg/mL are negative. However, beta-glucan does not detect mucormycosis, cryptococcus, or blastomyces. Treatment for invasive fungal infections typically needs to continue for an extended period. The recommended treatment duration is at least 2 weeks after the first negative test. In some cases, treatment is required for 1-3 months.
Here are some simple memory rules for antifungal treatment in invasive fungal infection.
- Fluconazole (Diflucan, Fluconazole) – for the treatment of candida albicans infections
Dosage: 800 mg on day 1. Maintenance dose: 400 mg once daily
- Cancidas (caspofungin) – for candida glabrata or resistance to Fluconazole
Dosage: A 70 mg single loading dose should be administered on day 1, followed by 50 mg daily. For patients weighing more than 80 kg, after the initial 70 mg loading dose, 70 mg daily is recommended.
- Vfend (voriconazole) – for invasive aspergillosis
Dosage: Loading dose: 400 mg every 12 hours on the first day, then 200 mg every 12 hours
- Mycamine (micafungin) – like Cancidas: invasive candidiasis
Dosage: 100 mg/day
- Noxafil (posaconazole) – given orally/parenterally. Invasive aspergillus infection.
Dosage: 300 mg x 2 on day 1. Maintenance dose: 300 mg once daily
- Ecalta (anidulafungin) – primarily for liver or kidney failure. Invasive candidiasis.
Dosage: A starting dose of 200 mg should be given on day 1, followed by 100 mg per day thereafter.
- Cresemba (isavuconazonium) – invasive aspergillosis, mucormycosis.
Dosage: 200 mg x 3 should be given on days 1-2, followed by 200 mg per day thereafter.
- AmBisome (Amphotericin B) – severe systemic and deep fungal infections.
AmBisome liposomal should be administered as an intravenous infusion over 30-60 minutes. Start treatment with 3 to 5 mg/kg, administered daily for at least 14 days.
