Author:
Kai Knudsen
Updated:
18 February, 2026
An overview of pediatric pain management, including assessment tools, age-appropriate analgesics, regional techniques, dosing principles, and safe perioperative strategies for children.
- Pain management in children
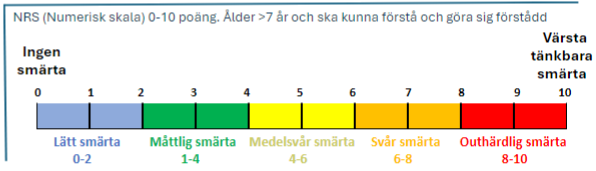
- Pain assessment scale for children 0–7 years
- FLACC – Face, Legs, Activity, Cry, Consolability
- Face, Legs, Activity, Cry, Consolability 0–10 points, children 0–18 years
- AS facial scale
- COMFORT-B pain assessment in children
- Newborns and infants
- Non-pharmacological pain relief in infants
- Non-pharmacological pain relief in preschool/school-aged children
- Peripheral Analgesics
- Intubated children – pharmacological baseline treatment
- Medications for pain relief and sedation in children
- Morphine and Other Strong Analgesics for Children
- Regional anesthesia
Pain management in children

Pain assessment scale for children 0–7 years
FLACC – Face, Legs, Activity, Cry, Consolability
For pain assessment in children aged 0–7 years, a behavioral pain assessment scale is used. It can also be used for children with multiple disabilities.
- Observe the child for a few minutes and then assess the categories face/legs/activity/cry/consolability to determine whether a score of 0, 1, or 2 applies.
- Then sum the points; the maximum score is 10.
- A value of < 3 is desirable. At values < 4, nursing interventions may be sufficient; at values > 4, pain relief should be considered.
- Whenever pain is suspected and nursing interventions do not help the child, a trial of analgesic administration should be performed. Evaluate the result with pain assessment.
Face, Legs, Activity, Cry, Consolability 0–10 points, children 0–18 years
| FLACC (0–10 points, 0–18 years) | 0 | 1 | 2 |
|---|---|---|---|
| Face | Neutral facial expression or smiles | Occasional frown, withdrawn, disinterested | Frequent or constant frown, quivering chin, clenched jaw |
| Legs | Normal position or relaxed | Uneasy, restless, or tense | Kicking or legs drawn up |
| Activity | Lying quietly, normal position, moves easily | Squirming, shifting position frequently, tense | Arched, jerking, or rigid |
| Cry | No cry (awake or asleep) | Moans or whimpers, occasional complaint | Persistent crying, screaming or sobbing, frequent complaints |
| Consolability | Content, relaxed | Reassured by touching, holding, or talking; distractible | Difficult to console or comfort |
AS facial scale

AS is a modified VAS scale for children aged 5–18 years. It consists of six faces; the first face corresponds to 0 points and the sixth face to 10 points. At 4 points or higher, pain relief should be considered. Keep in mind that some children may confuse emotional states with pain. Do not ask “Does it hurt?” Instead ask “Do you feel anything from the wound?” If the answer is yes, ask “How does it feel?” If the child confirms pain, ask “How much does it hurt?” and “Can you show it on the scale?”
The facial scale is an analogue of the Faces Pain Scale (FPS; Bieri et al., Pain 41 (1990) 139).
COMFORT-B pain assessment in children
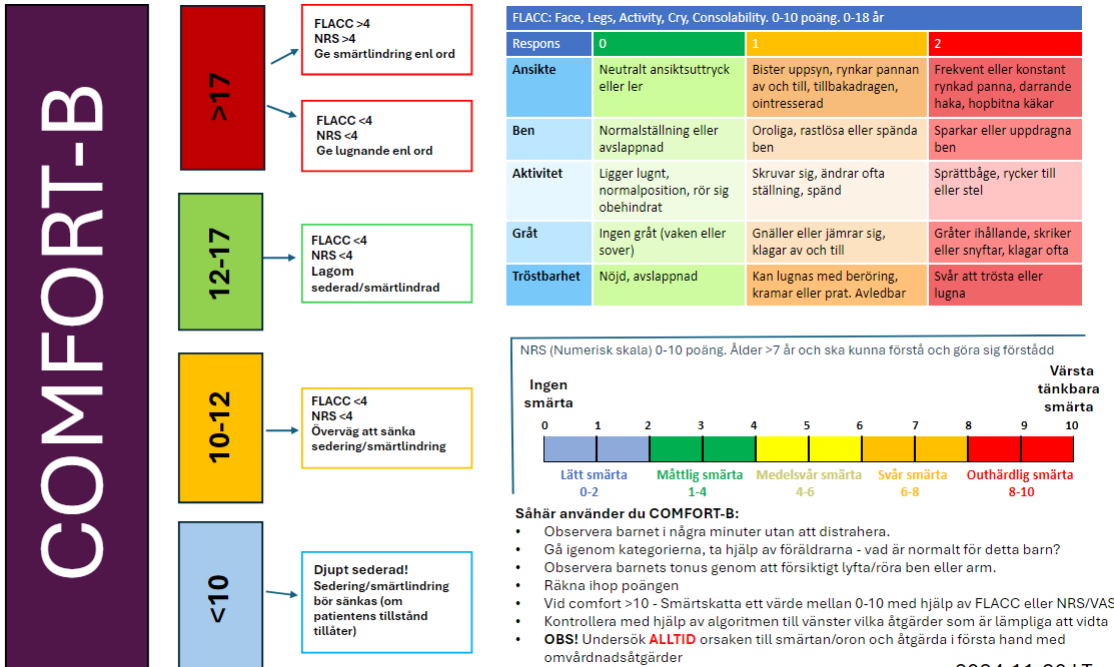
How to use COMFORT-B:
- Observe the child for a few minutes without distracting them.
- Go through the categories and involve the parents – what is normal for this child?
- Assess the child’s muscle tone by gently lifting/moving a leg or arm.
- Calculate the total score.
- If COMFORT-B > 10: Assess pain on a scale from 0–10 using FLACC or NRS/VAS.
- Check the algorithm on the left to determine appropriate interventions.
- NOTE! ALWAYS investigate the cause of pain/anxiety and primarily address it with nursing interventions.
Basic pain treatment
Newborns and infants
A calm newborn/infant is not always adequately pain relieved!
- Inadequately pain-relieved infants may become passive over time with reduced movements, expressionless facial appearance, decreased heart rate and oxygen saturation
- Distinguish between pain/hunger/abdominal discomfort
Non-pharmacological pain relief in infants
- Support the child’s attempts at self-regulation
- Skin-to-skin contact
- Sucking on a pacifier or finger ± sugar
- Parents
Non-pharmacological pain relief in preschool/school-aged children
- Explain and prepare according to age (e.g. demonstrate on a doll)
- Distraction (tablet, soap bubbles)
- Older children: autonomy – e.g. lie down or sit?
- Parents
Peripheral Analgesics

- Ketorolac (Toradol®) 0.3 mg/kg x 4 iv (not < 3-6 months, COX 1+2)
- Parecoxib (Dynastat®) 0.5 mg/kg x 1 iv (not < 3-6 months COX 2)
- Ibuprofen 7.5 mg/kg x 3-4 po (not < 3 months COX 1+2)
- Paracetamol po 15 mg/kg x 4 (first 3 days 20-25 mg/kg x 4)
- Paracetamol iv 15 mg/kg x 4 (use iv primarily the first postoperative day)
Intubated children – pharmacological baseline treatment
Baseline sedation
- Infusion of morphine/oxycodone + infusion/intermittent clonidine/dexdor
- Note: children <3 months have a risk of accumulation of opioids and midazolam. Reduce the dose after a few hours of loading
Additional PRN:
- 0–1 month: midazolam infusion
- 1–12 months: Propofol <24 h, otherwise midazolam
- Over 12 months: Propofol
Briefly on tolerance and tapering
- Opioid rotation every 1 week with morphine/oxycodone infusion, conversion factor 1:1.
- If treatment >5 days (also applies to midazolam): reduce by 15–20% per day.
- If treatment exceeds 9 days: reduce by 10% per day.
- If reducing midazolam and opioid simultaneously: reduce each drug by 15% per day.
- At low doses (morphine 5 microg/kg/h, midazolam 0.05 mg/kg/h), switch to oral formulation.
Sedative agents:
- Ketamine/Esketamine
- Phenobarbital (Fenemal) (note accumulation; check serum levels after 2–3 days of treatment)
Analgesic agents:
- Ketamine/esketamine
- Methadone (adjunct in high-dose opioid use >5 days or during tapering)
Medications for pain relief and sedation in children
| Drug | Type of drug and receptor binding | Indication and dosing | Prolonged half-life | Additional information |
|---|---|---|---|---|
| Alfentanil | Short-acting opioid, ~20× more potent than IV morphine | Procedure-related pain 5–10 µg/kg | 1) Liver failure 2) Children 0–3 months | Risk of apnea and chest wall rigidity (especially in infants) |
| Dexmedetomidine | Short-acting α2-adrenoceptor agonist | Sedation Infusion 0.3–1.4 µg/kg/h | 1) Liver failure 2) Children 0–3 months | Risk of bradycardia Avoid in patients with AV block II–III without pacemaker |
| Esketamine | S-enantiomer of racemic ketamine, NMDA receptor antagonist | Sedation, analgesia Infusion 0.1–0.25 (up to 0.6) mg/kg/h | 1) Liver failure 2) Children 0–3 months | Increased airway secretions Risk of agitation and hallucinations – attenuated by other sedatives |
| Phenobarbital | Long-acting barbiturate, CNS depression via GABA-A receptors | Sedation, injection 5 mg/kg (max 100 mg per dose, up to 3 doses per day) | 1) Liver failure 2) Children 0–1 month | Induces hepatic CYP450 enzymes, may increase metabolism of warfarin |
| Fentanyl | Opioid, ~100× more potent than IV morphine | Procedure-related pain Infusion 0.5–1 µg/kg | 1) Liver failure 2) Children 0–3 months | Risk of apnea and chest wall rigidity (especially in infants) Tachycardia during infusion |
| Ketamine | R+S ketamine (racemate), S-enantiomer is NMDA receptor antagonist | Sedation, analgesia Infusion 0.2–0.5 (up to 1) mg/kg/h | 1) Liver failure 2) Children 0–3 months | Increased airway secretions Risk of hallucinations and agitation – attenuated by other sedatives |
| Clonidine | α2-adrenoceptor agonist (inhibits pain signal transmission to the brain) | Sedation, analgesia Infusion 0.5–2 µg/kg/h Injection 1–2 µg/kg alt. Oral 2–3 µg/kg x4–8 | 1) Renal failure 2) Children 0–1 month | Risk of bradycardia and hypotension at higher doses |
| Melatonin | Pineal hormone involved in circadian rhythm regulation | 1–4 years: 1–2 mg 5–18 years: 2–5 mg | Administer 60–90 minutes before desired sleep | |
| Methadone | Long-acting opioid, also NMDA receptor antagonist (reduces opioid tolerance) | Opioid tapering Severe chronic pain Dose: see methadone chapter | Liver failure | Long half-life Highly variable pharmacokinetics (newborns–adults) Multiple drug interactions Risk of QT prolongation |
| Midazolam | Benzodiazepine, GABA-A receptor agonist | Sedation Infusion 0.05–0.2 mg/kg/h Prefer oral route during tapering | 1) Renal failure 2) Liver failure 3) Children 0–3 months | Respiratory depression Increased risk of ICU delirium Absorbed in ECMO circuit |
| Morphine | Opioid | Analgesia Infusion 5–30 µg/kg/h | 1) Renal failure 2) Liver failure 3) Children 0–3 months | Newborns: large variability in half-life |
| Oxycodone | Opioid, equi-potent to IV morphine | Analgesia Infusion 5–30 µg/kg/h | 1) Liver failure 2) Children 0–3 months | |
| Propofol | Anesthetic agent, probably via GABA receptors | Sedation Infusion intubated: 1–4 mg/kg/h Spontaneous breathing: 0.5–2 mg/kg/h | Children 0–1 month | 0–2 months: preferably avoid infusion 2–12 months: max infusion 24 h |
Morphine and Other Strong Analgesics for Children
Morphine for postoperative pain in Pediatric Use
| Age | Loading dose morphine (mg/kg) | Cont. infusion morphine (μg/kg/h) |
|---|---|---|
| 0 - 3 months | 0.05 | 5-15 |
| 3 - 12 months | 0.1 | 10-20 |
| 1 - 5 years | 0.15 | 10 - 40 |
| 6 -12 years | 0.2 | 10 - 40 |
| 12 - 16 years | 0.25 | 10 - 40 |
Dosage of Morphine for Children
| Morphine | 1 mg/ml i v |
|---|---|
| Age | Dosage |
| <3 months | 50 µg/kg (0,05 mg/kg = 0,05 ml/kg of morphine 1 mg/ml) |
| 3-12 months | 100 µg/kg (0,1 mg/kg = 0,1 ml/kg of morphine 1 mg/ml) |
| 1-5 years | 150 µg/kg (0,15 mg/kg = 0,15 ml/kg of morphine 1 mg/ml) |
| 5-12 years | 200 µg/kg (0,20 mg/kg = 0,20 ml of morphine 1 mg/ml) |
| 12-15 years | 250 µg/kg (0,25 mg/kg = 0,25 ml/kg of morphine 1 mg/ml) |
Oxicodon for children (postoperative pain treatment)
| Oxicodon (Oxynorm) | 1 mg/ml |
|---|---|
| Oral solution | 0.1-0.2 mg/kg (max. 10 mg) up to 4 times/day |
| Given for severe opioid-sensitive pain. | ATTENTION! At least one hour of monitoring after the last dose! |

Fentanyl for children
| Fentanyl | 50 µg/ml (0.05 mg/ml) |
|---|---|
| Intravenously | 1 µg/kg |
| In continuous infusion for sedation in the ICU | 0,5-1 μg/kg/hour |
| Nasally | > 3 years 1,5 µg/kg |
Intravenous naloxone dosage for children (Nexodal®)
| Naloxone iv | Dosage 2 µg/kg | The dose can be repeated if necessary |
|---|---|---|
| Weight (kg) | Solution 20 µg/ml | Solution 0.4 mg/ml (children > 20 kg) |
| 3-5 kg | 0,3-0,5 ml | |
| 5-10 kg | 0,5-1,0 ml | |
| 10-20 kg | 1,0-2,0 ml | |
| 20-40 kg | 2,0-4,0 ml | 0,1-0,2 ml |
| 40-80 kg | 4,0-8,0 ml | 0,2-0,4 ml |
Regional anesthesia
- Spinal: Marcain spinal®: 0,3-0,4 mg/kg
- Sacral: Ropivacaine 1-2 mg/kg
- EPI (1-12 years): Ropivacaine (Naropin)
- Bolus: 2 mg/kg
- Infusion 0,4-1 mg/kg/h
Disclaimer:
The content on AnesthGuide.com is intended for use by medical professionals and is based on practices and guidelines within the Swedish healthcare context.
While all articles are reviewed by experienced professionals, the information provided may not be error-free or universally applicable.
Users are advised to always apply their professional judgment and consult relevant local guidelines.
By using this site, you agree to our Terms of Use.
